

Myocardial Tissue Characterization in Heart Failure with Preserved Ejection Fraction: From Histopathology and Cardiac Magnetic Resonance Findings to Therapeutic Targets
- PMID: 34299270
- PMCID: PMC8304780
- DOI: 10.3390/ijms22147650
Myocardial Tissue Characterization in Heart Failure with Preserved Ejection Fraction: From Histopathology and Cardiac Magnetic Resonance Findings to Therapeutic Targets
Abstract
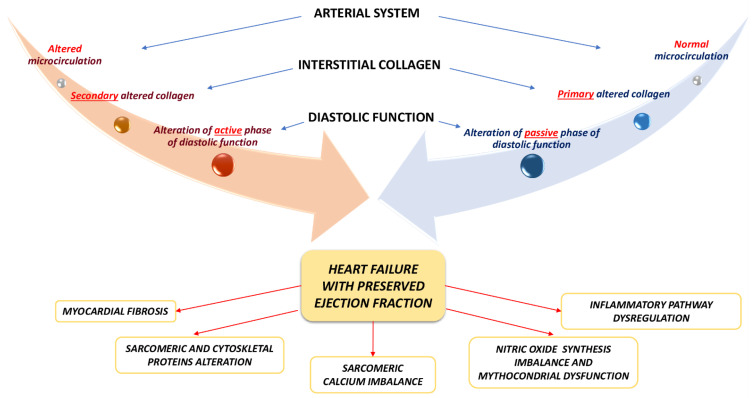
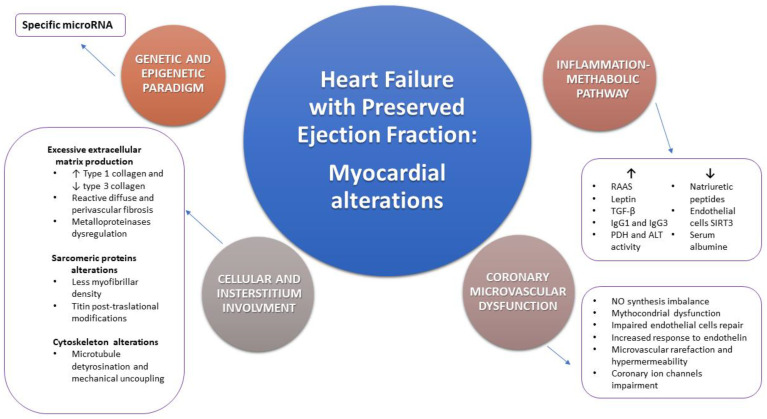
Heart failure with preserved ejection fraction (HFpEF) is a complex clinical syndrome responsible for high mortality and morbidity rates. It has an ever growing social and economic impact and a deeper knowledge of molecular and pathophysiological basis is essential for the ideal management of HFpEF patients. The association between HFpEF and traditional cardiovascular risk factors is known. However, myocardial alterations, as well as pathophysiological mechanisms involved are not completely defined. Under the definition of HFpEF there is a wide spectrum of different myocardial structural alterations. Myocardial hypertrophy and fibrosis, coronary microvascular dysfunction, oxidative stress and inflammation are only some of the main pathological detectable processes. Furthermore, there is a lack of effective pharmacological targets to improve HFpEF patients' outcomes and risk factors control is the primary and unique approach to treat those patients. Myocardial tissue characterization, through invasive and non-invasive techniques, such as endomyocardial biopsy and cardiac magnetic resonance respectively, may represent the starting point to understand the genetic, molecular and pathophysiological mechanisms underlying this complex syndrome. The correlation between histopathological findings and imaging aspects may be the future challenge for the earlier and large-scale HFpEF diagnosis, in order to plan a specific and effective treatment able to modify the disease's natural course.
Keywords: cardiac magnetic resonance; endomyocardial biopsy; heart failure; heart failure with preserved ejection fraction; myocardial tissue characterization; therapy.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
-
- Mureddu G.F., Agabiti N., Rizzello V., Forastiere F., Latini R., Cesaroni G., Masson S., Cacciatore G., Colivicchi F., Uguccioni M., et al. Prevalence of preclinical and clinical heart failure in the elderly. A population-based study in Central Italy. Eur. J. Heart Fail. 2012;14:718–729. doi: 10.1093/eurjhf/hfs052. - DOI - PubMed
-
- Ponikowski P., Voors A.A., Anker S., Bueno H., Cleland G.F.J., Coats A.J.S., Falk V., González-Juanatey J.R., Harjola V.P., Jankowska E.A., et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
-
- Gerber Y., Weston S.A., Redfield M.M., Chamberlain A.M., Manemann S.M., Jiang R., Killian J.M., Roger V.L. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010. JAMA Intern Med. 2015;175:996–1004. doi: 10.1001/jamainternmed.2015.0924. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
