

X Chromosome Inactivation in Carriers of Fabry Disease: Review and Meta-Analysis
- PMID: 34299283
- PMCID: PMC8304911
- DOI: 10.3390/ijms22147663
X Chromosome Inactivation in Carriers of Fabry Disease: Review and Meta-Analysis
Abstract
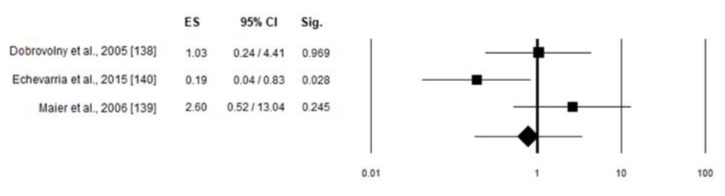
Anderson-Fabry disease is an X-linked inborn error of glycosphingolipid catabolism caused by a deficiency of α-galactosidase A. The incidence ranges between 1: 40,000 and 1:117,000 of live male births. In Italy, an estimate of incidence is available only for the north-western Italy, where it is of approximately 1:4000. Clinical symptoms include angiokeratomas, corneal dystrophy, and neurological, cardiac and kidney involvement. The prevalence of symptomatic female carriers is about 70%, and in some cases, they can exhibit a severe phenotype. Previous studies suggest a correlation between skewed X chromosome inactivation and symptoms in carriers of X-linked disease, including Fabry disease. In this review, we briefly summarize the disease, focusing on the clinical symptoms of carriers and analysis of the studies so far published in regards to X chromosome inactivation pattern, and manifesting Fabry carriers. Out of 151 records identified, only five reported the correlation between the analysis of XCI in leukocytes and the related phenotype in Fabry carriers, in particular evaluating the Mainz Severity Score Index or cardiac involvement. The meta-analysis did not show any correlation between MSSI or cardiac involvement and skewed XCI, likely because the analysis of XCI in leukocytes is not useful for predicting the phenotype in Fabry carriers.
Keywords: Fabry disease; X chromosome inactivation; carriers.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Desnick R.J., Brady R., Barranger J., Collins A.J., Germain D.P., Goldman M., Grabowski G., Packman S., Wilcox W.R. Fabry disease, an under-recognized multisystemic disorder: Expert recommendations for diagnosis, management, and enzyme replacement therapy. Ann. Intern. Med. 2003;138:338–346. doi: 10.7326/0003-4819-138-4-200302180-00014. - DOI - PubMed
-
- Scriver C.R., Beaudet A.L., Sly W.S., Valle D., Childs B., Kinzler K.W., Vogelstein B. The Metabolic and Molecular Bases of Inherited Disease. 8th ed. McGraw-Hill; New York, NY, USA: 2001.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
