

Is loss of smell an early predictor of COVID-19 severity: a systematic review and meta-analysis
- PMID: 34302637
- PMCID: PMC8302975
- DOI: 10.1007/s12272-021-01344-4
Is loss of smell an early predictor of COVID-19 severity: a systematic review and meta-analysis
Abstract
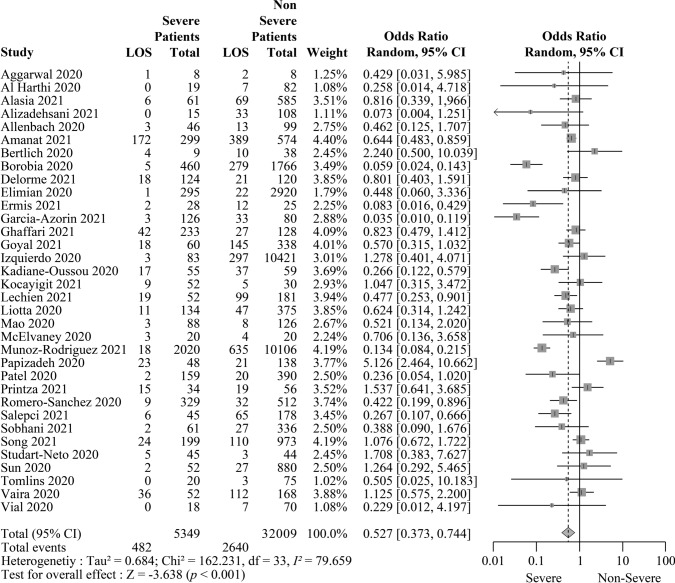
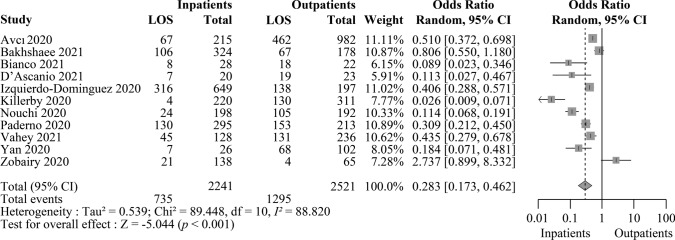
Anecdotal evidence suggests that the severity of coronavirus disease of 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is likely to be distinguished by variations in loss of smell (LOS). Thus, we conducted a meta-analysis of 45 articles that include a total of 42,120 COVID-19 patients from 17 different countries to demonstrate that severely ill or hospitalized COVID-19 patients have a lesser chance of experiencing LOS than non-severely ill or non-hospitalized COVID-19 patients (odds ratio = 0.527 [95% CI 0.373-0.744; p < 0.001] and 0.283 [95% CI 0.173-0.462; p < 0.001], respectively). We also proposed a possible mechanism underlying the association of COVID-19 severity with anosmia, which may explain why patients without sense of smell develop severe COVID-19. Variations in LOS according to the severity of COVID-19 is a global phenomenon, with few exceptions. Since severely ill patients have a lower rate of anosmia, patients without anosmia should be monitored more closely in the early stages of COVID-19, for early diagnosis of severity of illness. An understanding of how the severity of COVID-19 infection and LOS are associated has profound implications for the clinical management and mitigation strategies for the disease.
Keywords: Anosmia; COVID-19; COVID-19 hospitalization; COVID-19 severity; SARS-CoV-2.
© 2021. The Pharmaceutical Society of Korea.
Conflict of interest statement
The authors declare that they have no conflicts of interests.
Figures


References
-
- Aggarwal S, Garcia-Telles N, Aggarwal G, Lavie C, Lippi G, Henry BM. Clinical features, laboratory characteristics, and outcomes of patients hospitalized with coronavirus disease 2019 (COVID-19): Early report from the United States. Diagnosis (berl) 2020;7:91–96. doi: 10.1515/dx-2020-0046. - DOI - PubMed
-
- Al Harthi S, Magdi A, Al Ruwaida I, Al Sultan L, Bina K, Al Mustafa S, Al Nasser K, Al Salim Q, Al Mohamed H, Al Hamad H, Al Thamra G (2020) Clinical characteristics of confirmed cases of COVID-19 admitted at Al-Nahdha hospital, Oman: a cross-sectional descriptive study. Preprint at 10.21203/rs.3.rs-39988/v1 - PMC - PubMed
-
- Alasia D, Owhonda G, Maduka O, Nwadiuto I, Arugu G, Tobin-West C, Azi E, Oris-Onyiri V, Urang IJ, Abikor V, Olofinuka AM, Adebiyi O, Somiari A, Avundaa H, Alali A. Clinical and epidemiological characteristics of 646 hospitalised SARS-Cov-2 positive patients in Rivers State Nigeria: a prospective observational study. Pan Afr Med J. 2021;38:25. doi: 10.11604/pamj.2021.38.25.26755. - DOI - PMC - PubMed
-
- Alizadehsani R, Alizadeh Sani Z, Behjati M, Roshanzamir Z, Hussain S, Abedini N, Hasanzadeh F, Khosravi A, Shoeibi A, Roshanzamir M, Moradnejad P, Nahavandi S, Khozeimeh F, Zare A, Panahiazar M, Acharya UR, Islam SMS. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J Med Virol. 2021;93:2307–2320. doi: 10.1002/jmv.26699. - DOI - PMC - PubMed
-
- Allenbach Y, Saadoun D, Maalouf G, Vieira M, Hellio A, Boddaert J, Gros H, Salem JE, Resche Rigon M, Menyssa C, Biard L, Benveniste O, Cacoub P. Development of a multivariate prediction model of intensive care unit transfer or death: a French prospective cohort study of hospitalized COVID-19 patients. PLoS ONE. 2020;15:e0240711. doi: 10.1371/journal.pone.0240711. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
