

Healthcare-associated infection impact with bioaerosol treatment and COVID-19 mitigation measures
- PMID: 34302883
- PMCID: PMC8295046
- DOI: 10.1016/j.jhin.2021.07.006
Healthcare-associated infection impact with bioaerosol treatment and COVID-19 mitigation measures
Abstract
Background: The real-world impact of breathing zone air purification and coronavirus disease 2019 (COVID-19) mitigation measures on healthcare-associated infections is not well documented. Engineering solutions to treat airborne transmission of disease may yield results in controlled test chambers or single rooms, but have not been reported on hospital-wide applications, and the impact of COVID-19 mitigation measures on healthcare-associated infection rates is unknown.
Aim: To determine the impact of hospital-wide bioaerosol treatment and COVID-19 mitigation measures on clinical outcomes.
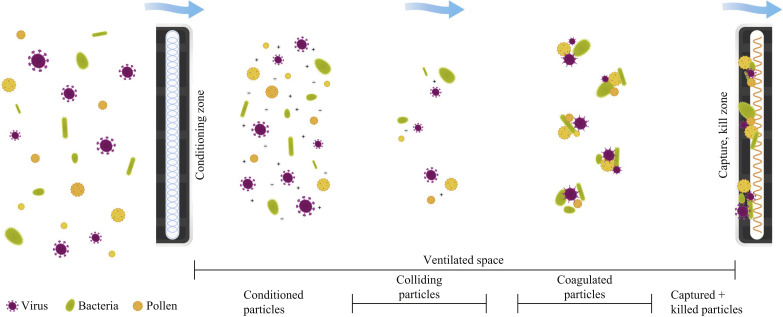
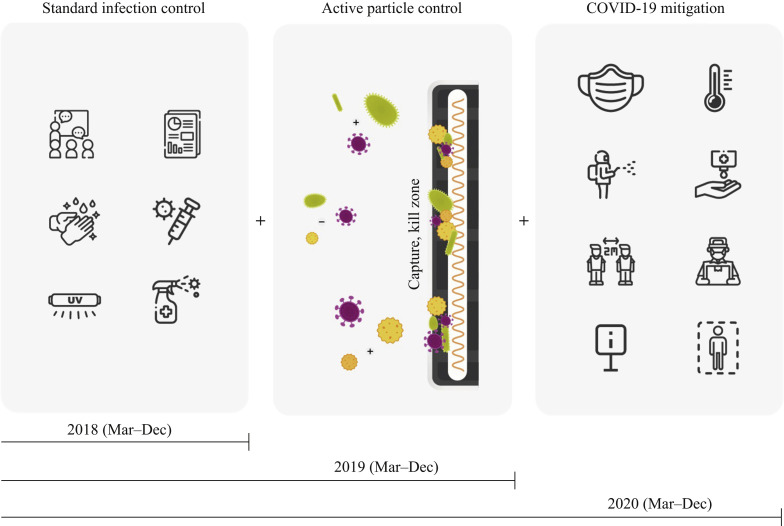
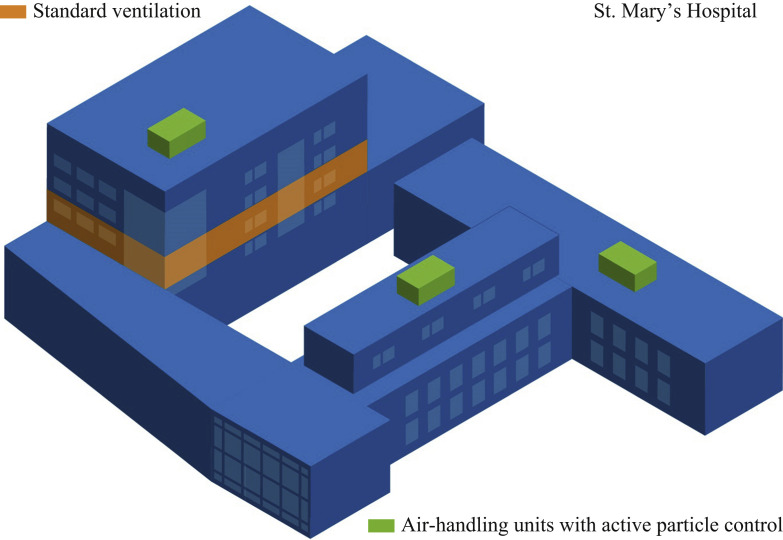
Methods: The impact of the step-wise addition of air disinfection technology and COVID-19 mitigation measures to standard multi-modal infection control on particle counts, viral and bacterial bioburden, and healthcare-associated infection rates was investigated in a 124-bed hospital (>100,000 patient-days over 30 months).
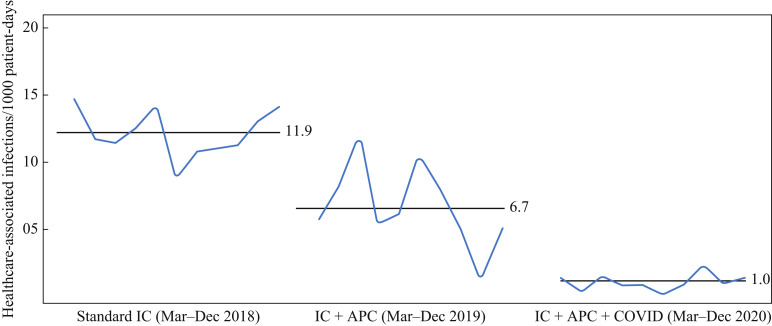
Findings and conclusion: The addition of air disinfection technology and COVID-19 mitigation measures reduced airborne ultrafine particles, altered hospital bioburden, and reduced healthcare-associated infections from 11.9 to 6.6 (per 1000 patient-days) and from 6.6 to 1.0 (per 1000 patient-days), respectively (P<0.0001, R2=0.86). No single technology, tool or procedure will eliminate healthcare-associated infections, but the addition of a ubiquitous facility-wide engineering solution at limited expense and with no alteration to patient, visitor or staff traffic or workflow patterns reduced infections by 45%. A similar impact was documented with the addition of comprehensive, restrictive, and labour- and material-intensive COVID-19 mitigation measures. To the authors' knowledge, this is the first direct comparison between traditional infection control, an engineering solution and COVID-19 mitigation measures.
Keywords: Aerosol transmission; Aerosolization; COVID-19; Disease transmission; Engineering; Healthcare-associated infections.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Bischoff W.E., Swett K., Leng I., Peters T.R. Exposure to influenza virus aerosols during routine patient care. J Infect Dis. 2013;207:1037–1046. - PubMed
-
- Bourouiba L. Turbulent gas clouds and respiratory pathogen emissions: potential implications for reducing transmission of COVID-19. JAMA. 2020;323:1837–1838. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
