

French recommendations for the management of systemic sclerosis
- PMID: 34304732
- PMCID: PMC8310704
- DOI: 10.1186/s13023-021-01844-y
French recommendations for the management of systemic sclerosis
Abstract
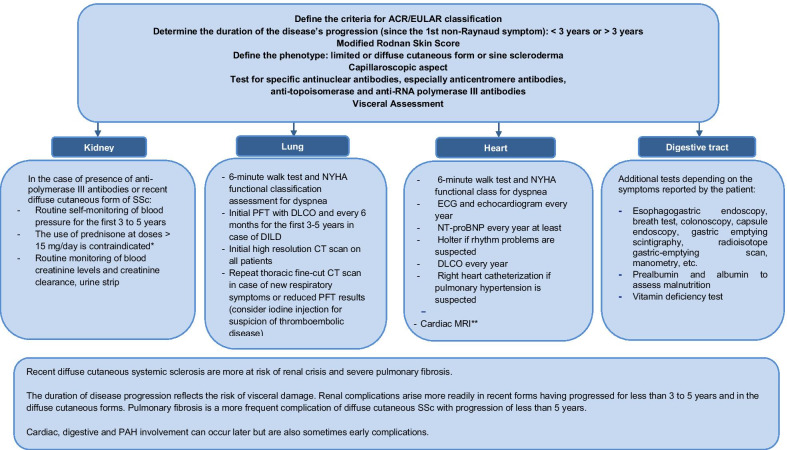
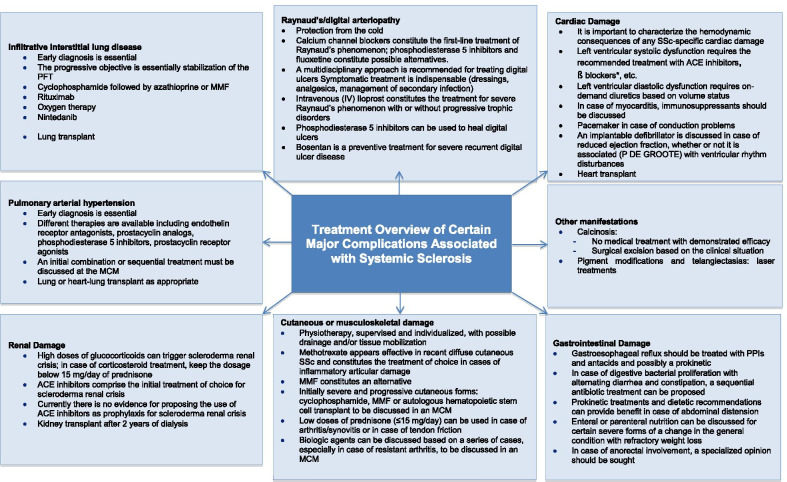
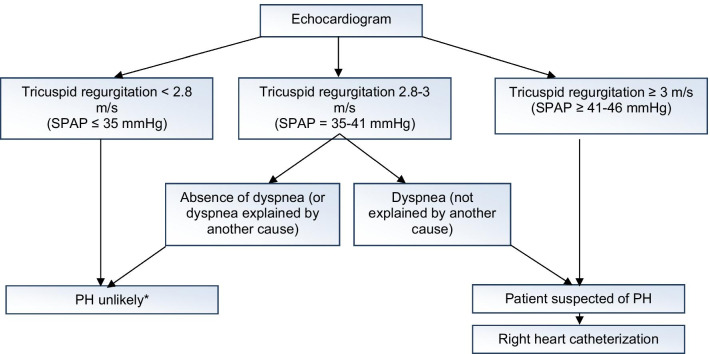
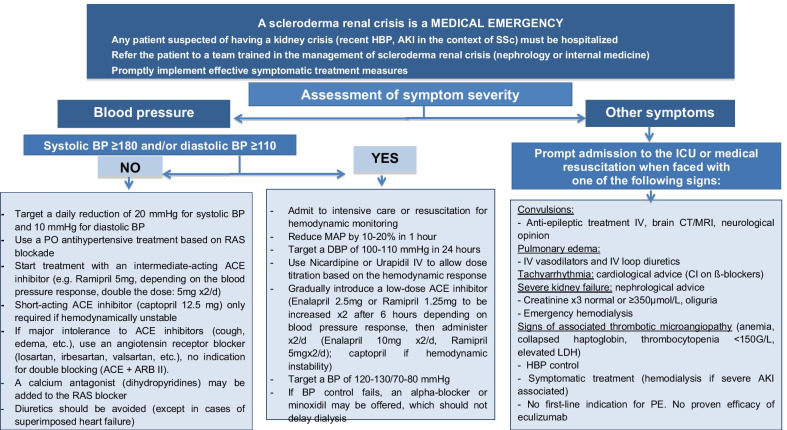
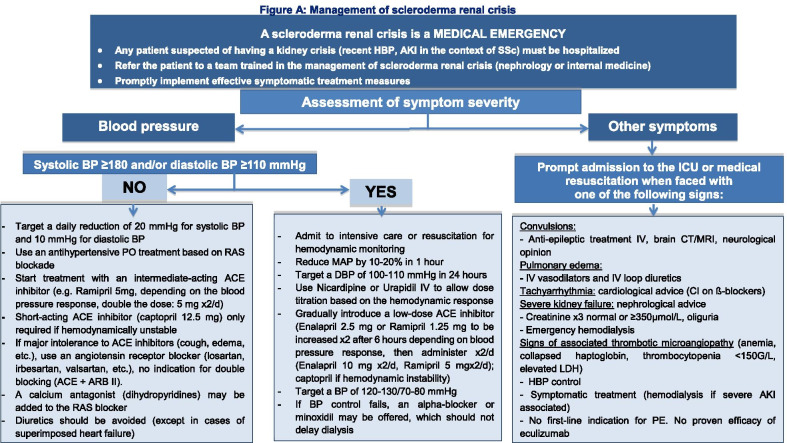
Systemic sclerosis (SSc) is a generalized disease of the connective tissue, arterioles, and microvessels, characterized by the appearance of fibrosis and vascular obliteration. There are two main phenotypical forms of SSc: a diffuse cutaneous form that extends towards the proximal region of the limbs and/or torso, and a limited cutaneous form where the cutaneous sclerosis only affects the extremities of the limbs (without passing beyond the elbows and knees). There also exists in less than 10% of cases forms that never involve the skin. This is called SSc sine scleroderma. The prognosis depends essentially on the occurrence of visceral damage and more particularly interstitial lung disease (which is sometimes severe), pulmonary arterial hypertension, or primary cardiac damage, which represent the three commonest causes of mortality in SSc. Another type of involvement with poor prognosis, scleroderma renal crisis, is rare (less than 5% of cases). Cutaneous extension is also an important parameter, with the diffuse cutaneous forms having less favorable prognosis.
Keywords: Recommendations; Systemic sclerosis; Treatment.
© 2021. The Author(s).
Conflict of interest statement
EH reports consulting fees/meeting fees from Actelion, Boehringer Ingelheim, Bayer, GSK, Roche-Chugai, Sanofi-Genzyme; speaking fees from Actelion, GSK, Roche-Chugai; and research funding from Octapharma, CSL Behring, GSK, Roche-Chugai and Actelion. CA reports no conflicts of interest. YA reports consulting fees/meeting fees from Actelion, Sanofi; Boehringer, Inventiva, Roche, Bayer, Sandoz, Medac, BMS; and research funding from Pfizer, BMS, Sandoz, Roche, Inventiva and Sanofi. JA reports no conflicts of interest. BBM reports no conflicts of interest. ABELOT reports no conflicts of interest. ABEREZNE reports no conflicts of interest. ASB reports no conflicts of interest. GW reports no conflicts of interest. JC reports no conflicts of interest. PDG reports consulting fees/meeting fees from Actelion, Bayer, MSD; speaking fees from Actelion, BAYER. ED reports consulting fees/meeting fees from Actelion. FD reports no conflicts of interest. PJ reports no conflicts of interest. FJ reports no conflicts of interest. DL reports no conflicts of interest. VL reports consulting fees/meeting fees from GSK and Astra-Zeneca. JSL reports no conflicts of interest. GL reports no conflicts of interest. CM reports no conflicts of interest. BM reports no conflicts of interest. CN reports no conflicts of interest. NO reports no conflicts of interest. FP reports no conflicts of interest. MAR reports no conflicts of interest. JR reports no conflicts of interest. AR reports no conflicts of interest. OS reports no conflicts of interest. VS reports no conflicts of interest. MET reports consulting fees/meeting fees from UCB, Lilly, Abbvie, MSD, Pfizer, Medac, Roche, Novartis, and BMS. LM reports no conflicts of interest.
Figures
References
-
- Avouac J, Allanore Y. Targeted immunotherapies in systemic sclerosis. Clin Exp Rheumatol. 2014;32(2 Suppl 81):165–172. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
