

Imaging Modalities for Evaluation of Intestinal Obstruction
- PMID: 34305469
- PMCID: PMC8292005
- DOI: 10.1055/s-0041-1729737
Imaging Modalities for Evaluation of Intestinal Obstruction
Abstract
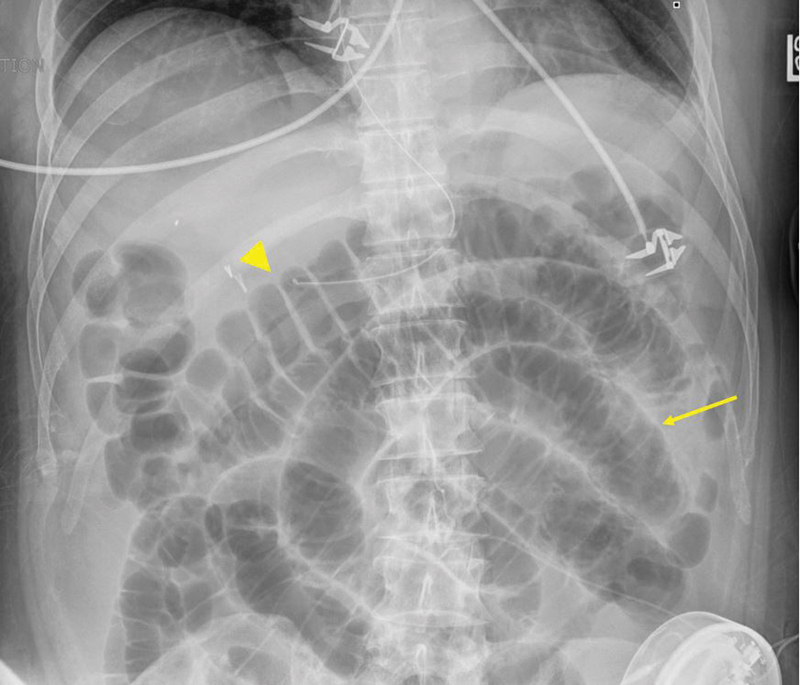
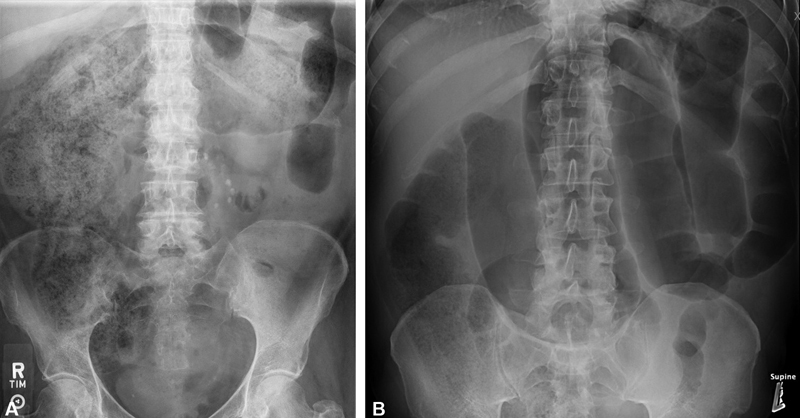
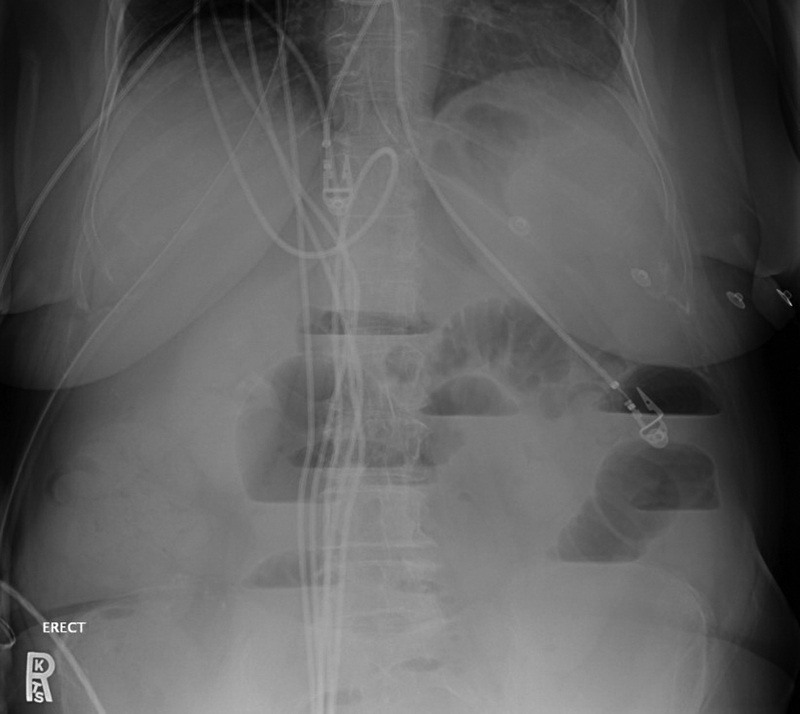
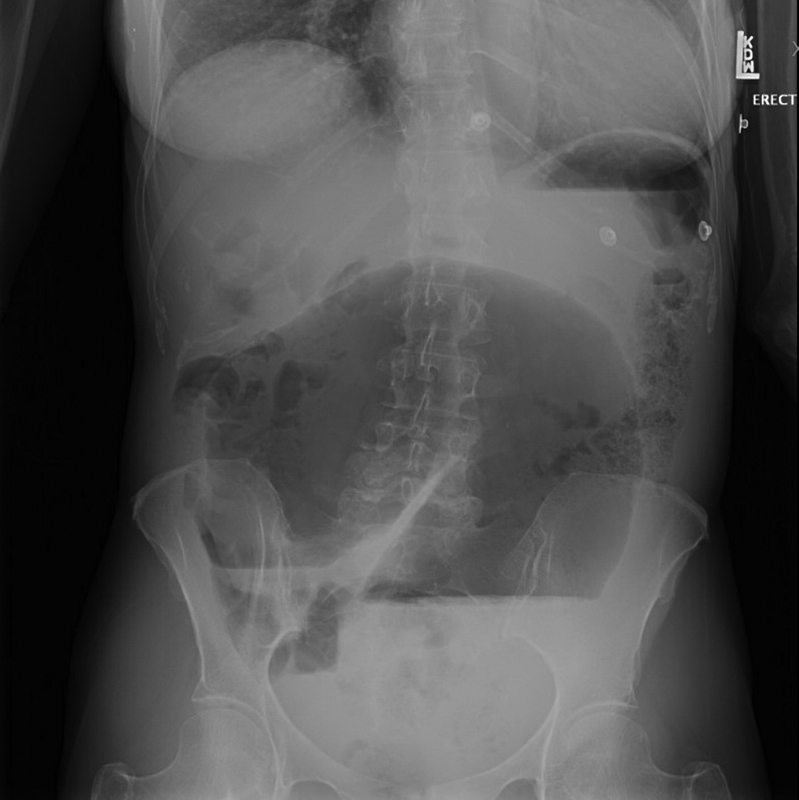
It is essential for the colon and rectal surgeon to understand the evaluation and management of patients with both small and large bowel obstructions. Computed tomography is usually the most appropriate and accurate diagnostic imaging modality for most suspected bowel obstructions. Additional commonly used imaging modalities include plain radiographs and contrast imaging/fluoroscopy, while less commonly utilized imaging modalities include ultrasonography and magnetic resonance imaging. Regardless of the imaging modality used, interpretation of imaging should involve a systematic, methodological approach to ensure diagnostic accuracy.
Keywords: abdominal radiography; bowel obstruction; computed tomography; contrast enema; imaging; large bowel obstruction; magnetic resonance imaging; small bowel follow-through; small bowel obstruction; ultrasound.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures



Similar articles
-
The diagnostic value of different imaging modalities in evaluation of bowel obstruction.Ann Univ Mariae Curie Sklodowska Med. 2004;59(2):268-74. Ann Univ Mariae Curie Sklodowska Med. 2004. PMID: 16146091
-
[Emergency radiology of bowel obstruction].Chirurg. 2006 Oct;77(10):889-97. doi: 10.1007/s00104-006-1232-1. Chirurg. 2006. PMID: 16960703 German.
-
Reliability and role of plain film radiography and CT in the diagnosis of small-bowel obstruction.AJR Am J Roentgenol. 1996 Dec;167(6):1451-5. doi: 10.2214/ajr.167.6.8956576. AJR Am J Roentgenol. 1996. PMID: 8956576
-
[Update: Small bowel diseases in computed tomography and magnetic resonance imaging].Radiologie (Heidelb). 2023 Jun;63(6):435-440. doi: 10.1007/s00117-023-01139-2. Epub 2023 Apr 4. Radiologie (Heidelb). 2023. PMID: 37016034 Review. German.
-
Comparative Effectiveness of Imaging Modalities for the Diagnosis of Intestinal Obstruction in Neonates and Infants:: A Critically Appraised Topic.Acad Radiol. 2016 May;23(5):559-68. doi: 10.1016/j.acra.2015.12.014. Epub 2016 Feb 5. Acad Radiol. 2016. PMID: 26857524 Review.
Cited by
-
Malignant Acute Colonic Obstruction: Multidisciplinary Approach for Endoscopic Management.Cancers (Basel). 2024 Feb 18;16(4):821. doi: 10.3390/cancers16040821. Cancers (Basel). 2024. PMID: 38398212 Free PMC article. Review.
-
Critical Appraisal of Plain Abdominal X-rays in Acute Abdomen: A Review.Cureus. 2025 Mar 11;17(3):e80420. doi: 10.7759/cureus.80420. eCollection 2025 Mar. Cureus. 2025. PMID: 40213758 Free PMC article. Review.
-
Pregnant patients requiring emergency general surgery: a scoping review of diagnostic and management strategies.Can J Surg. 2025 May 29;68(3):E190-E213. doi: 10.1503/cjs.001124. Print 2025 May-Jun. Can J Surg. 2025. PMID: 40441877 Free PMC article.
-
The "Little-Old-Lady's Hernia", Obturator Hernia: A Case Report and Literature Review.Case Rep Surg. 2024 Jun 18;2024:1039438. doi: 10.1155/2024/1039438. eCollection 2024. Case Rep Surg. 2024. PMID: 39015132 Free PMC article.
-
When Not to Operate on Acute Cases-A Surgeon's Perspective on Rapid Assessment of Emergency Abdominopelvic Computed Tomography.J Imaging. 2023 Sep 28;9(10):200. doi: 10.3390/jimaging9100200. J Imaging. 2023. PMID: 37888307 Free PMC article. Review.
References
-
- Yeo H L, Lee S W. Colorectal emergencies: review and controversies in the management of large bowel obstruction. J Gastrointest Surg. 2013;17(11):2007–2012. - PubMed
-
- Drożdż W, Budzyński P. Change in mechanical bowel obstruction demographic and etiological patterns during the past century: observations from one health care institution. Arch Surg. 2012;147(02):175–180. - PubMed
-
- Parikh J A, Ko C Y, Maggard M A, Zingmond D S. What is the rate of small bowel obstruction after colectomy? Am Surg. 2008;74(10):1001–1005. - PubMed
-
- Aberg H, Påhlman L, Karlbom U. Small-bowel obstruction after restorative proctocolectomy in patients with ulcerative colitis. Int J Colorectal Dis. 2007;22(06):637–642. - PubMed
