

Induction Therapy Prior to Surgical Resection for Patients Presenting with Locally Advanced Esthesioneuroblastoma
- PMID: 34306928
- PMCID: PMC8289526
- DOI: 10.1055/s-0039-3402026
Induction Therapy Prior to Surgical Resection for Patients Presenting with Locally Advanced Esthesioneuroblastoma
Abstract
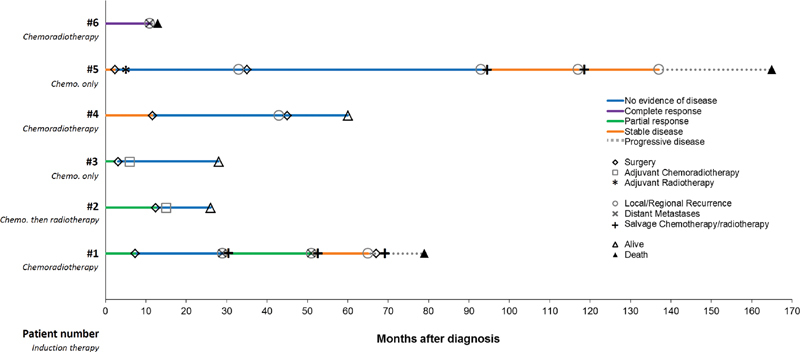
Esthesioneuroblastoma (ENB) is a rare olfactory malignancy that can present with locally advanced disease. At our institution, patients with ENB in whom the treating surgeon believes that a margin-negative resection is initially not achievable are selected to undergo induction with chemotherapy with or without radiotherapy prior to surgery. In a retrospective review of 61 patient records, we identified six patients (10%) treated with this approach. Five of six patients (83%) went on to definitive surgery. Prior to surgery, three of five patients (60%) had a partial response after induction therapy, whereas two of five (40%) had stable disease. Microscopically margin-negative resection was achieved in four of five (80%) of the patients who went on to surgery, while one patient had negative margins on frozen section but microscopically positive margins on permanent section. Three of five patients (60%) recurred after surgery; two of these patients died with recurrent/metastatic ENB. In summary, induction therapy may facilitate margin-negative resection in locally advanced ENB. Given the apparent sensitivity of ENB to chemotherapy and radiotherapy, future prospective studies should investigate the optimal multidisciplinary approach to improve long-term survival in this rare disease.
Keywords: esthesioneuroblastoma; induction; neoadjuvant; outcomes; therapy.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest A.V.C. reports funding for clinical trials from Merck, AstraZeneca/MedImmune, Kura Oncology, Inovio, Eisai (all institutional). The other authors report no relevant conflict of interest in submitting this article for publication.
Figures
References
-
- Dulguerov P, Allal A S, Calcaterra T C. Esthesioneuroblastoma: a meta-analysis and review. Lancet Oncol. 2001;2(11):683–690. - PubMed
-
- Broich G, Pagliari A, Ottaviani F.Esthesioneuroblastoma: a general review of the cases published since the discovery of the tumour in 1924 Anticancer Res 199717(4A):2683–2706. - PubMed
-
- Theilgaard S A, Buchwald C, Ingeholm P, Kornum Larsen S, Eriksen J G, Sand Hansen H. Esthesioneuroblastoma: a Danish demographic study of 40 patients registered between 1978 and 2000. Acta Otolaryngol. 2003;123(03):433–439. - PubMed
-
- Diaz E M, Jr, Johnigan R H, III, Pero C. Olfactory neuroblastoma: the 22-year experience at one comprehensive cancer center. Head Neck. 2005;27(02):138–149. - PubMed
