

Comprehensive Dissection of Treatment Patterns and Outcome for Patients With Metastatic Large-Cell Neuroendocrine Lung Carcinoma
- PMID: 34307143
- PMCID: PMC8295750
- DOI: 10.3389/fonc.2021.673901
Comprehensive Dissection of Treatment Patterns and Outcome for Patients With Metastatic Large-Cell Neuroendocrine Lung Carcinoma
Abstract
Background: Large-cell neuroendocrine lung carcinoma (LCNEC) is a rare pulmonary neoplasm with poor prognosis and limited therapeutic options.
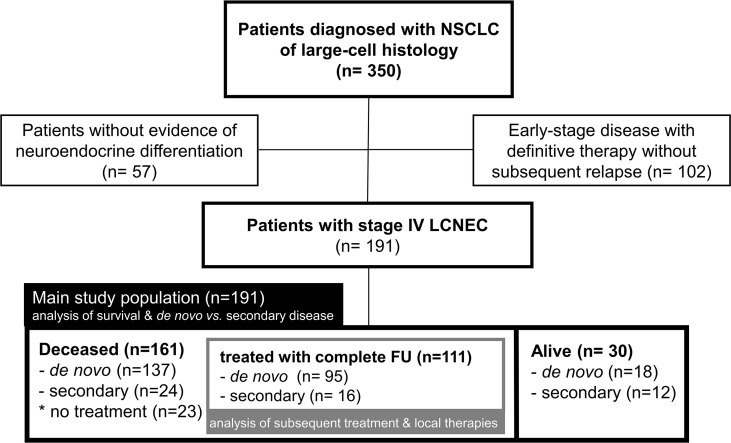
Methods: We retrospectively analyzed all patients with metastatic LCNEC in the records of a large German academic center since 2010.
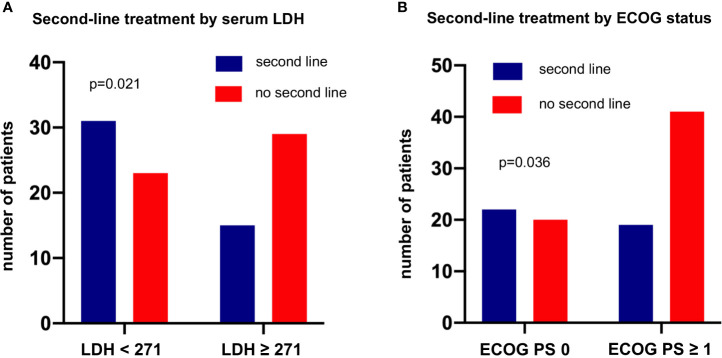
Results: 191 patients were identified with a predominance of male (68%) smokers (92%) and a median age of 65 years. The single most important factor associated with outcome was the type of systemic treatment, with a median overall survival (OS) of 26.4 months in case of immune checkpoint inhibitor administration (n=13), 9.0 months for other patients receiving first-line platinum doublets (n=129), and 4.0 months with non-platinum chemotherapies (n=17, p<0.01). Other patient characteristics independently associated with longer OS were a lower baseline serum LDH (hazard ratio [HR] 0.54, p=0.008) and fewer initial metastatic sites (HR 0.52, p=0.006), while the platinum drug type (cisplatin vs. carboplatin) and cytotoxic partner (etoposide vs. paclitaxel), patients' smoking status and baseline levels of tumor markers (NSE, CYFRA 21-1, CEA) did not matter. 12% (23/191) of patients forewent systemic treatment, mainly due to tumor-related clinical deterioration (n=13), while patient refusal of therapy (n=5) and severe concomitant illness (n=5) were less frequent. The attrition between successive treatment lines was approximately 50% and similar for platinum-based vs. other therapies, but higher in case of a worse initial ECOG status or higher serum LDH (p<0.05). 19% (36/191) of patients had secondary stage IV disease and showed fewer metastatic sites, better ECOG status and longer OS (median 12.6 vs. 8.7 months, p=0.030). Among the 111 deceased patients with palliative systemic treatment and complete follow-up, after exclusion of oligometastatic cases (n=8), administration of local therapies (n=63 or 57%) was associated with a longer OS (HR 0.58, p=0.008), but this association did not persist with multivariable testing.
Conclusions: Highly active systemic therapies, especially immunotherapy and platinum doublets, are essential for improved outcome in LCNEC and influence OS stronger than clinical disease parameters, laboratory results and other patient characteristics. The attrition between chemotherapy lines is approximately 50%, similar to other NSCLC. Patients with secondary metastatic disease have a more favorable clinical phenotype and longer survival.
Keywords: de novo metastatic; immunotherapy; large-cell neuroendocrine lung carcinoma; local therapies; overall survival; platinum chemotherapy; secondary metastatic.
Copyright © 2021 Fisch, Bozorgmehr, Kazdal, Kuon, Klotz, Shah, Eichhorn, Kriegsmann, Schneider, Muley, Stenzinger, Bischoff and Christopoulos.
Conflict of interest statement
FB reports research funding from BMS and travel grants from BMS and MSD. DK reports advisory board and speaker’s honoraria from AstraZeneca, BMS, Pfizer. JK reports research funding from AstraZeneca and Celgene. RS reports research funding from BMS and speaker’s honoraria from Roche. TM reports research funding from Roche and patents with Roche. AS reports advisory board honoraria from BMS, AstraZeneca, ThermoFisher, Novartis, speaker’s honoraria from BMS, Illumina, AstraZeneca, Novartis, ThermoFisher, MSD, Roche, and research funding from Chugai. PC reports research funding from AstraZeneca, Novartis, Roche, Takeda, and advisory board/lecture fees from AstraZeneca, Boehringer Ingelheim, Chugai, Novartis, Pfizer, Roche, Takeda. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Travis WD, Linnoila RI, Tsokos MG, Hitchcock CL, Cutler Jr GB, Nieman L, et al. . Neuroendocrine Tumors of the Lung With Proposed Criteria for Large-Cell Neuroendocrine Carcinoma. An Ultrastructural, Immunohistochemical, and Flow Cytometric Study of 35 Cases. Am J Surg Pathol (1991) 15:529–53. 10.1097/00000478-199106000-00003 - DOI - PubMed
-
- Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JH, Beasley MB, et al. . The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thor Oncol (2015) 10:1243–60. 10.1097/JTO.0000000000000630 - DOI - PubMed
LinkOut - more resources
Full Text Sources