

Giant androgen-producing adrenocortical carcinoma with atrial flutter: A case report and review of the literature
- PMID: 34307612
- PMCID: PMC8281402
- DOI: 10.12998/wjcc.v9.i20.5575
Giant androgen-producing adrenocortical carcinoma with atrial flutter: A case report and review of the literature
Abstract
Background: Adrenocortical carcinoma (ACC), the second most aggressive malignant tumor, lacks epidemiological data worldwide; therefore, every new case can improve the understanding of the pathology and treatment of this malignancy.
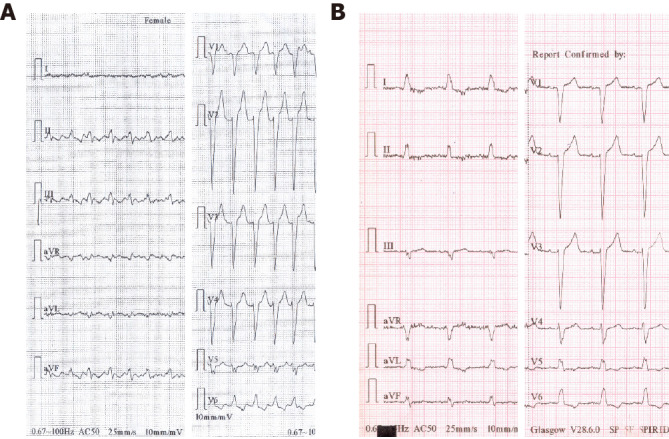
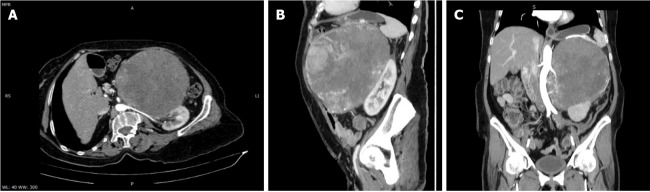
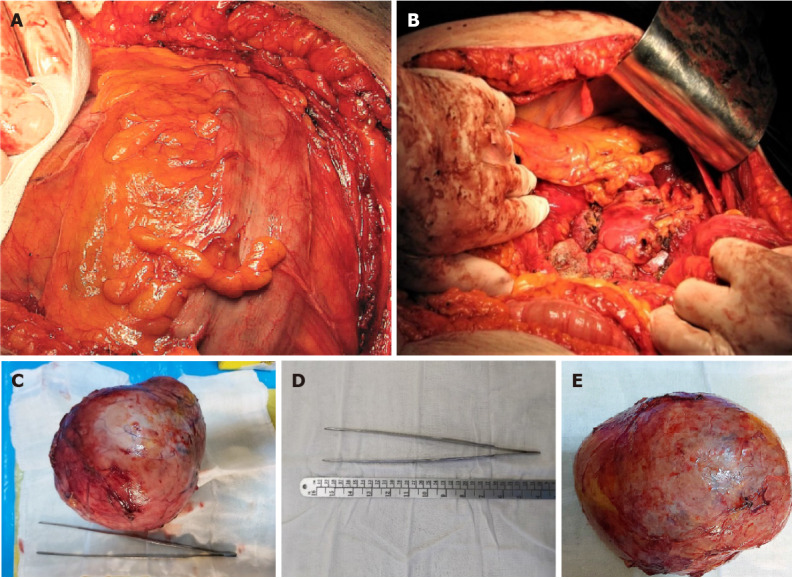
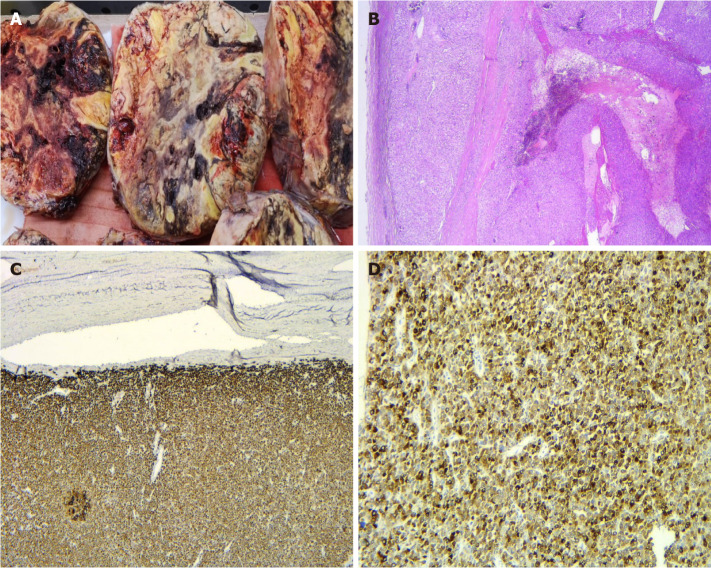
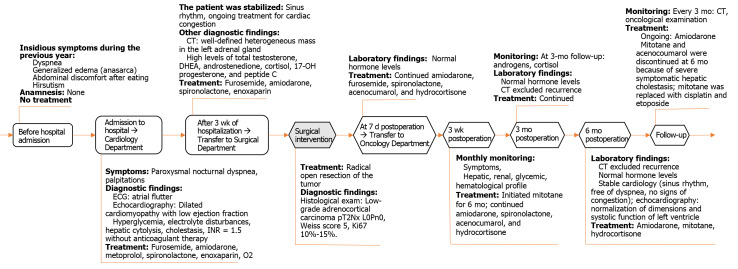
Case summary: We present the case of a 66-year-old Caucasian woman with a giant androgen-producing ACC (21 cm × 17 cm × 12 cm; 2100 g), without metastases, which unusually presented with an acute onset of atrial flutter and congestive heart failure. The cardiac complications observed in our case support the hypothesis that androgen excess in women is a cardiovascular risk factor. Androgen excess in women can be a rare cause of reversible dilated cardiomyopathy, therefore a comprehensive approach to the patient is essential to improve the recognition of androgen-secreting ACC. The atrial flutter was remitted after initiation of drug treatment during admission. The severe heart failure was totally remitted at 6 mo after radical open surgery to remove the giant ACC.
Conclusion: Radical open surgery to remove a giant androgen-producing ACC was the first-line treatment to cure the excess of androgen, which determined the total remission of cardiac complications at 6 mo after surgery in the women of this case report.
Keywords: Adrenalectomy; Adrenocortical carcinoma; Androgen secreting tumor; Atrial flutter; Case report; Heart failure.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures

Similar articles
-
Androgen secreting giant adrenocortical carcinoma with no metastases: A case report and review of the literature.Can Urol Assoc J. 2015 Sep-Oct;9(9-10):E644-7. doi: 10.5489/cuaj.2867. Epub 2015 Sep 9. Can Urol Assoc J. 2015. PMID: 26425231 Free PMC article.
-
An Interesting Case of Hepatic Adrenocortical Carcinoma.Acta Med Indones. 2018 Jul;50(3):257-259. Acta Med Indones. 2018. PMID: 30333277
-
Castration failure in prostate carcinoma due to a functioning adrenocortical carcinoma.Endocrinol Diabetes Metab Case Rep. 2021 Oct 1;2021:21-0036. doi: 10.1530/EDM-21-0036. Online ahead of print. Endocrinol Diabetes Metab Case Rep. 2021. PMID: 34673545 Free PMC article.
-
Giant nonfunctioning adrenal tumors: two case reports and review of the literature.J Med Case Rep. 2018 Nov 10;12(1):335. doi: 10.1186/s13256-018-1876-8. J Med Case Rep. 2018. PMID: 30413177 Free PMC article. Review.
-
Giant virilising adrenal cortical carcinoma.Autops Case Rep. 2021 May 6;11:e2021259. doi: 10.4322/acr.2021.259. eCollection 2021. Autops Case Rep. 2021. PMID: 34307221 Free PMC article. Review.
References
-
- Palomeque Jiménez A, Calzado Baeza S, Reyes Moreno M, Robayo-Soto PS. Carcinoma of the adrenal cortex giant. Acta Med Port. 2013;26:759. - PubMed
-
- Estévez Fernández S, Artime Rial M, Domínguez Comesaña E, Sánchez Santos R. Giant adrenal cortical carcinoma. Cir Esp. 2017;95:542. - PubMed
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH ESC Committee for Practice Guidelines. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Europace. 2010;12:1360–1420. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
