

Spinal vascular lesions: anatomy, imaging techniques and treatment
- PMID: 34307789
- PMCID: PMC8283341
- DOI: 10.1016/j.ejro.2021.100369
Spinal vascular lesions: anatomy, imaging techniques and treatment
Abstract
Background: Vascular lesions of the spinal cord are rare but potentially devastating conditions whose accurate recognition critically determines the clinical outcome. Several conditions lead to myelopathy due to either arterial ischemia, venous congestion or bleeding within the cord. The clinical presentation varies, according with the different aetiology and mechanism of damage.
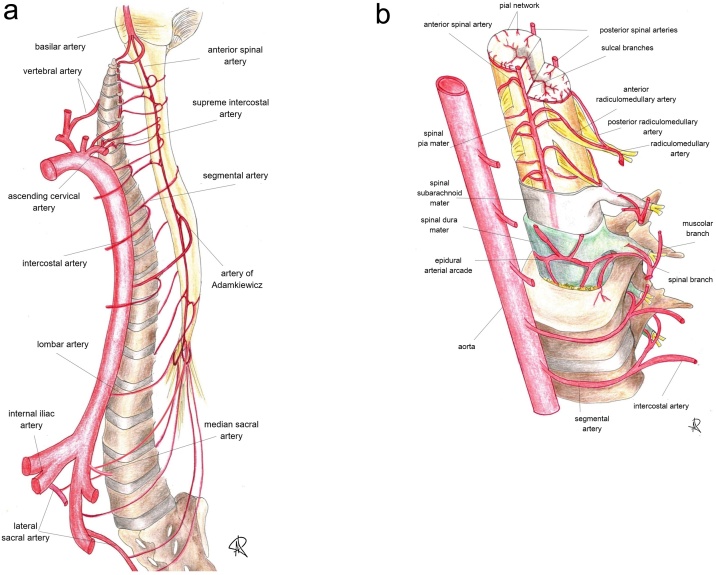
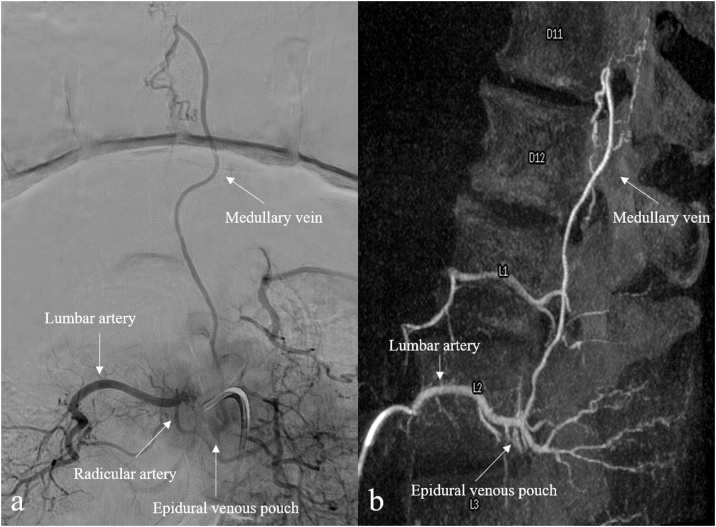
Purpose: The aim is to provide a comprehensive review on the radiological features of the most common vascular myelopathies, passing through the knowledge of the vascular spinal anatomy and the clinical aspects of the different aetiologies, which is crucial to promptly address the diagnosis and the radiological assessment.
Keywords: MRI; Neuroimaging; Spinal angiography; Spinal cord anatomy; Vascular myelopathies; Vascular spinal cord lesions.
© 2021 The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures













References
Publication types
LinkOut - more resources
Full Text Sources
