

Chronic Inflammation in Chronic Kidney Disease Progression: Role of Nrf2
- PMID: 34307974
- PMCID: PMC8258499
- DOI: 10.1016/j.ekir.2021.04.023
Chronic Inflammation in Chronic Kidney Disease Progression: Role of Nrf2
Abstract
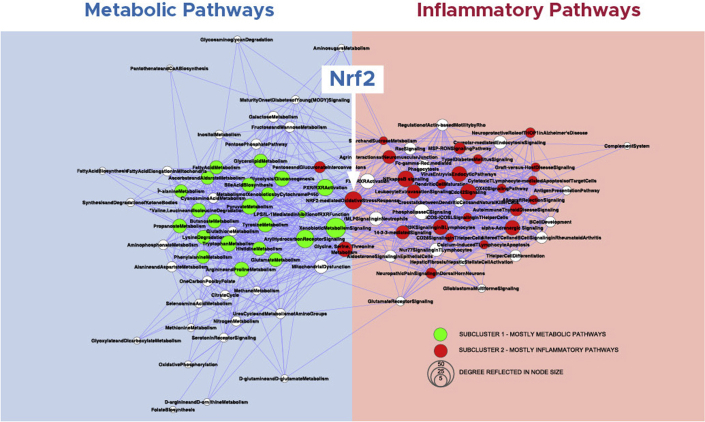
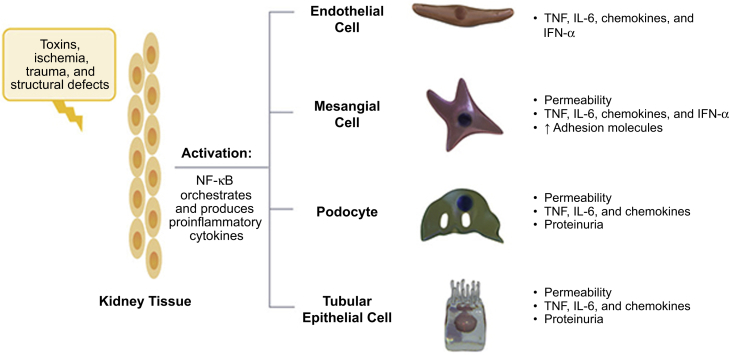
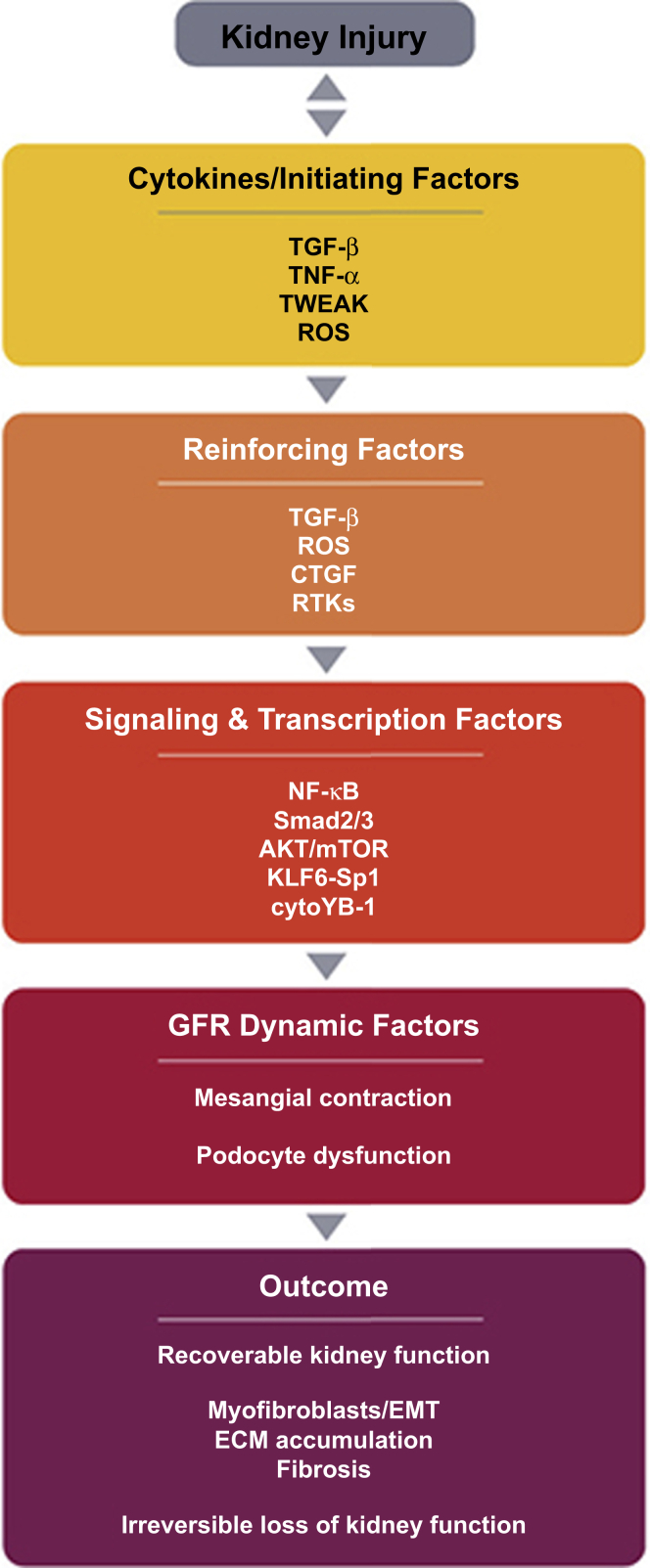
Despite recent advances in the management of chronic kidney disease (CKD), morbidity and mortality rates in these patients remain high. Although pressure-mediated injury is a well-recognized mechanism of disease progression in CKD, emerging data indicate that an intermediate phenotype involving chronic inflammation, oxidative stress, hypoxia, senescence, and mitochondrial dysfunction plays a key role in the etiology, progression, and pathophysiology of CKD. A variety of factors promote chronic inflammation in CKD, including oxidative stress and the adoption of a proinflammatory phenotype by resident kidney cells. Regulation of proinflammatory and anti-inflammatory factors through NF-κB- and nuclear factor, erythroid 2 like 2 (Nrf2)-mediated gene transcription, respectively, plays a critical role in the glomerular and tubular cell response to kidney injury. Chronic inflammation contributes to the decline in glomerular filtration rate (GFR) in CKD. Whereas the role of chronic inflammation in diabetic kidney disease (DKD) has been well-elucidated, there is now substantial evidence indicating unresolved inflammatory processes lead to fibrosis and eventual end-stage kidney disease (ESKD) in several other diseases, such as Alport syndrome, autosomal-dominant polycystic kidney disease (ADPKD), IgA nephropathy (IgAN), and focal segmental glomerulosclerosis (FSGS). In this review, we aim to clarify the mechanisms of chronic inflammation in the pathophysiology and disease progression across the spectrum of kidney diseases, with a focus on Nrf2.
Keywords: Nrf2; chronic inflammation; chronic kidney disease; mitochondrial dysfunction; oxidative stress; resident kidney cells.
© 2021 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Helal I., Fick-Brosnahan G.M., Reed-Gitomer B., Schrier R.W. Glomerular hyperfiltration: definitions, mechanisms and clinical implications. Nat Rev Nephrol. 2012;8:293–300. - PubMed
-
- Noone D., Licht C. An update on the pathomechanisms and future therapies of Alport syndrome. Pediatr Nephrol. 2013;28:1025–1036. - PubMed
-
- Wright J.T., Jr., Bakris G., Greene T. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: results from the AASK trial. JAMA. 2002;288:2421–2431. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
