

Chronic diseases, health conditions and risk of COVID-19-related hospitalization and in-hospital mortality during the first wave of the epidemic in France: a cohort study of 66 million people
- PMID: 34308411
- PMCID: PMC8282330
- DOI: 10.1016/j.lanepe.2021.100158
Chronic diseases, health conditions and risk of COVID-19-related hospitalization and in-hospital mortality during the first wave of the epidemic in France: a cohort study of 66 million people
Abstract
Background: From the beginning of the COVID-19 pandemic, age (most importantly), male gender and various comorbidities were found to be associated with severe forms of COVID-19. However, there was little information provided for an entire country such as France, which was severely affected throughout the epidemic.
Methods: In France, the SNDS, comprising all health insurance reimbursements and benefits, and the PMSI, comprising hospital data, can be used to estimate the risk associated with about fifty diseases or health conditions for hospitalization primarily related to COVID-19 and COVID-19-related deaths. A cohort was constituted comprising all people alive on February 15, 2020. Data were censored at 15 June 2020 for COVID-19-related hospitalization and at 15 July 2020 for death for patients still hospitalized for COVID-19 on 15 June 2020. Cox proportional hazards models were used to estimate hazard ratios (HR) for the associations between each comorbidity (n=47) and the risk of COVID-19-related hospitalization or death. These associations were determined with adjustment for age and gender, and then in models including all variables (adjusted hazard ratios [aHR]).
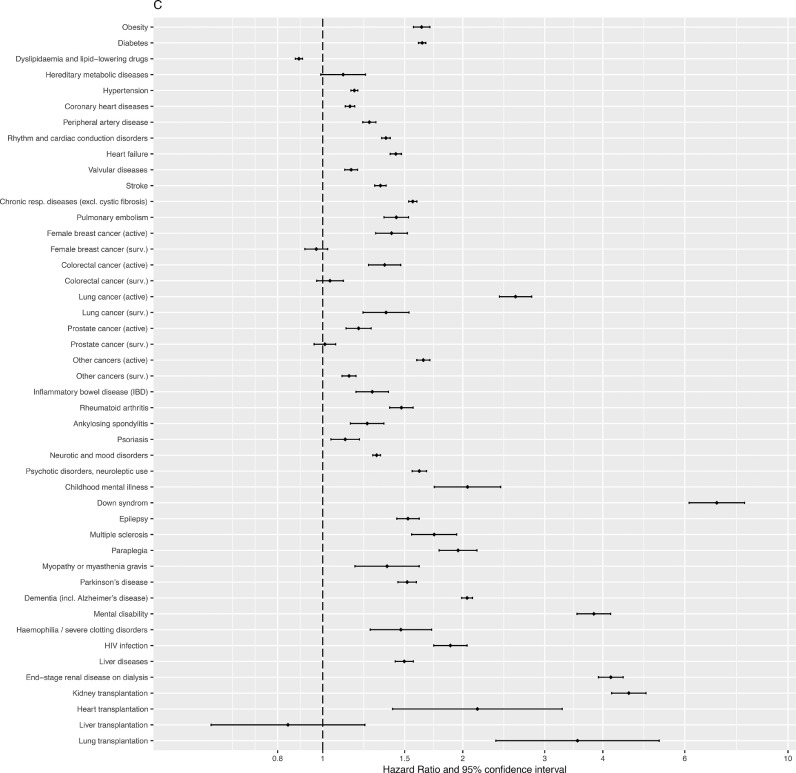
Findings: In a population of 66,050,090 people, 87,809 people (134 per 100,000) were hospitalized for COVID-19 between February 15, 2020 and June 15, 2020 and a subgroup of 15,661 people (24 per 100,000) died in hospital.A much higher risk was observed with increasing age, reaching a risk of hospitalization for COVID-19 more than five fold higher and a risk of COVID-19-related in-hospital mortality more than 100-fold higher in people aged 85 years and older (absolute risks of 750 and 268 per 100,000, respectively) compared to people aged 40 to 44 years.Men were at higher risk of COVID-19-related hospitalization aHR 1.38 [1.36-1.40]) and COVID-19-related in-hospital mortality (aHR 2.08 [2.01-2.16]) compared to women. Positive associations between social deprivation index and risk of COVID-19 were also observed. Almost all chronic health conditions were positively associated with an increased risk of COVID-19-related hospitalization and in-hospital mortality, with the exception of dyslipidaemia, which was negatively associated. The strongest associations for both COVID-19-related hospitalization and in-hospital mortality were observed in people with Down syndrome (7.0 [6.1-8.1] and 22.9 [17.1-30.7], respectively), mental retardation (3.8 [3.5-4.2] and 7.3 [6.1-8.8], respectively), kidney transplantation (4.6 [4.2-5.0] and 7.1 [6.0-8.4], respectively), lung transplantation (3.5 [2.4-5.3] and 6.2 [2.8-14.0], respectively) end-stage renal disease on dialysis (4.2 [3.9-4.4] and 4.7 [4.2-5.2], respectively) and active lung cancer (2.6 [2.4-2.8] and 4.0 [3.5-4.6], respectively).
Interpretation: This national cohort study confirms the associations with most diseases and health conditions in France and provides data on less frequent health conditions, which could be useful particularly to target priority populations during present and future vaccination campaigns.
Funding: None.
Keywords: COVID-19; death; hospitalization; medical factors; sociodemographic factors.
© 2021 The Authors.
Conflict of interest statement
All authors declare no conflict of interest.
Figures








References
LinkOut - more resources
Full Text Sources
