

Presentation and Outcomes of Infants With Idiopathic Cholestasis: A Multicenter Prospective Study
- PMID: 34310436
- PMCID: PMC8448404
- DOI: 10.1097/MPG.0000000000003248
Presentation and Outcomes of Infants With Idiopathic Cholestasis: A Multicenter Prospective Study
Abstract
Objectives: The aim of the study was to determine the frequency and natural history of infantile idiopathic cholestasis (IC) in a large, prospective, multicenter cohort of infants.
Methods: We studied 94 cholestatic infants enrolled up to 6 months of age in the NIDDK ChiLDReN (Childhood Liver Disease Research Network) "PROBE" protocol with a final diagnosis of IC; they were followed up to 30 months of age.
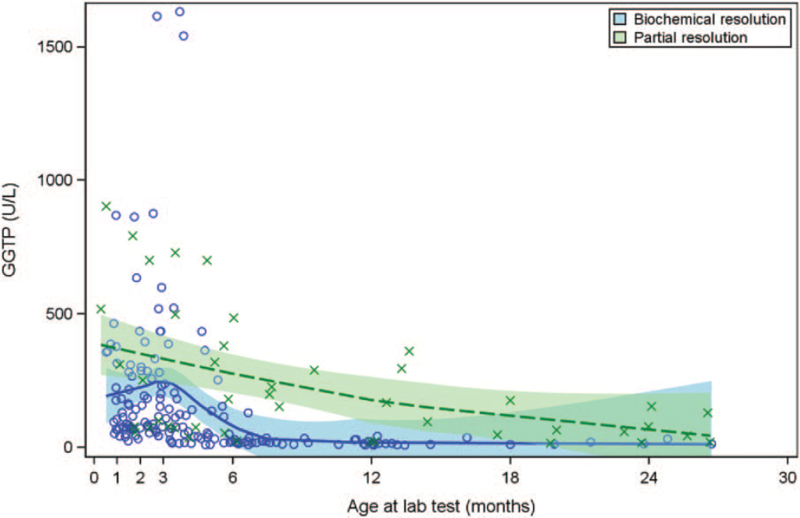
Results: Male sex (66/94; 70%), preterm birth (22/90 with data; 24% born at < 37 weeks' gestational age), and low birth weight (25/89; 28% born at <2500 g) were frequent, with no significant differences between outcomes. Clinical outcomes included death (n = 1), liver transplant (n = 1), biochemical resolution (total bilirubin [TB] ≤1 mg/dL and ALT < 35 U/L; n = 51), partial resolution (TB > 1 mg/dL and/or ALT > 35 U/L; n = 7), and exited healthy (resolved disease per study site report but without documented biochemical resolution; n = 34). Biochemical resolution occurred at median of 9 months of age. GGT was <100 U/L at baseline in 34 of 83 participants (41%).
Conclusions: Frequency of IC and of death or liver transplant was less common in this cohort than in previously published cohorts, likely because of recent discovery and diagnosis of genetic etiologies of severe/persistent cholestasis that previously were labeled as idiopathic. Preterm birth and other factors associated with increased vulnerability in neonates are relatively frequent and may contribute to IC. Overall outcome in IC is excellent. Low/normal GGT was common, possibly indicating a role for variants in genes associated with low-GGT cholestasis-this warrants further study.
Trial registration: ClinicalTrials.gov NCT00061828.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
Figures


References
-
- Balistreri WF, Bezerra JA. Whatever happened to “neonatal hepatitis”? Clin Liver Dis 2006; 10:27–53. - PubMed
-
- Lee WS, Chai PF, Boey CM, et al. . Aetiology and outcome of neonatal cholestasis in Malaysia. Singapore Med J 2010; 51:434–439. - PubMed
-
- Roberts EA. Neonatal hepatitis syndrome. Semin Neonatol 2003; 8:357–374. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 DK062481/DK/NIDDK NIH HHS/United States
- U01 DK062470/DK/NIDDK NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- U01 DK062436/DK/NIDDK NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- U01 DK062452/DK/NIDDK NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- U01 DK062466/DK/NIDDK NIH HHS/United States
- U01 DK084575/DK/NIDDK NIH HHS/United States
- U01 DK062456/DK/NIDDK NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- U01 DK103149/DK/NIDDK NIH HHS/United States
- U24 DK062456/DK/NIDDK NIH HHS/United States
- UL1 TR000130/TR/NCATS NIH HHS/United States
- U01 DK103140/DK/NIDDK NIH HHS/United States
- UL1 TR001872/TR/NCATS NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- U01 DK084538/DK/NIDDK NIH HHS/United States
- U01 DK062453/DK/NIDDK NIH HHS/United States
- U01 DK062503/DK/NIDDK NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- P30 DK078392/DK/NIDDK NIH HHS/United States
- U01 DK103135/DK/NIDDK NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- U01 DK084536/DK/NIDDK NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR001855/TR/NCATS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- U01 DK062500/DK/NIDDK NIH HHS/United States
- U01 DK062497/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
