

Ultrasound evaluation of access complications: Thrombosis, aneurysms, pseudoaneurysms and infections
- PMID: 34313154
- PMCID: PMC8607320
- DOI: 10.1177/11297298211018062
Ultrasound evaluation of access complications: Thrombosis, aneurysms, pseudoaneurysms and infections
Abstract
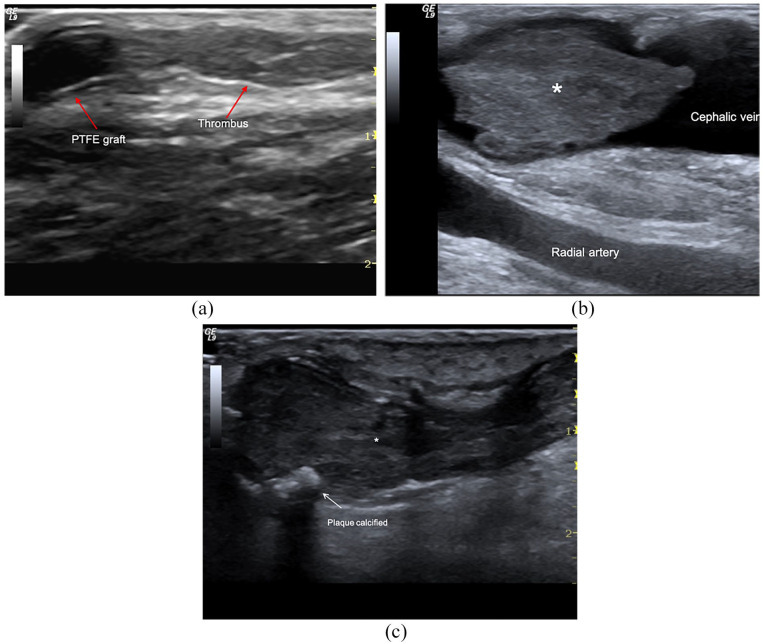
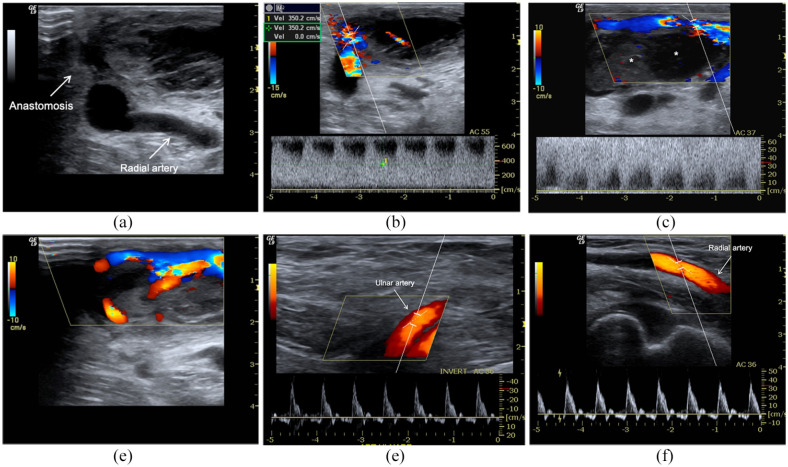
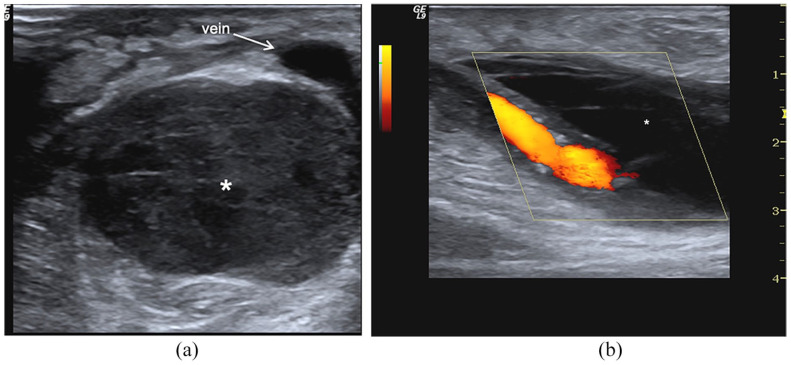
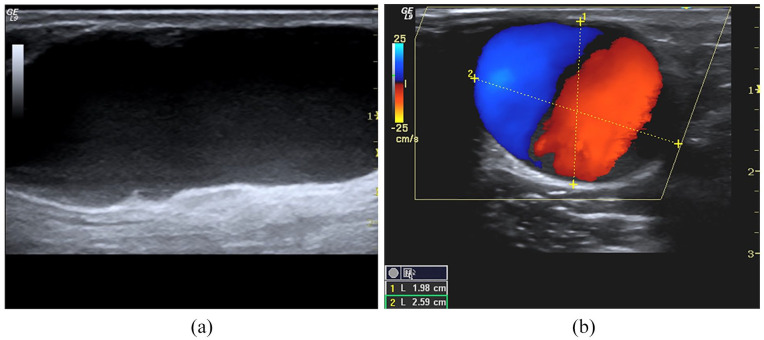
Arteriovenous fistula (AVF) complications are classified based on fistula outcomes. This review aims to update colour Doppler (CD) and pulse wave Doppler (PWD) roles in managing early and late complications of the native and prosthetic AVF. Vascular access (VA) failure occurs because inflow or outflow stenosis activates Wirchow's triad inducing thrombosis. Therefore, the diagnosis of the tributary artery and outgoing vein stenosis will be the first topic considered. Post-implantation complications occur from the inability to achieve AVF maturation and dialysis suitability due to inflow/outflow stenosis. Late stenosis is usually a sequence of early defects repaired to maintain patency. Less frequently, in the mature AVF or graft, complications are acquired 'de novo'. They derive either from incorrect management of vascular access (haematoma, pseudoaneurysm, prosthesis infection) or wall pathologies (aneurysm, myxoid valve degeneration, kinking, coiling, abnormal dilation from defects of elastic structures). High-resolution transducers (10-20 MHz) allow the characterization of the wall damage, haemodynamic dysfunctions, early and late complications even if phlebography remains the gold standard for the diagnosis for its sensitivity and specificity.
Keywords: AVF complications; doppler imaging; fistula aneurysm; inflow/outflow stenosis; pseudoaneurysm; vascular access thrombosis.
Conflict of interest statement
Figures
References
-
- Gallieni M, Hollenbeck M, Inston N, et al.. Clinical practice guideline on peri- and postoperative care of arteriovenous fistulas and grafts for haemodialysis in adults. Nephrol Dial Transplant 2019; 34(Supplement 2): ii1–ii42. - PubMed
-
- Schmidli J, Widmer MK, Basile C, et al.. Editor’s choice - vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55: 757–818. - PubMed
-
- McGrogan D, Al Shakarchi J, Khawaja A, et al.. Arteriovenous fistula outcomes in the elderly. J Vasc Surg 2015; 62:1652–1657. - PubMed
-
- Roy-Chaudhury P, Spergel LM, Besarab A, et al.. Biology of arteriovenous fistula failure. J Nephrol 2007; 20:150–163. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
