

Diagnostic performance rates of the ACR-TIRADS and EU-TIRADS based on histopathological evidence
- PMID: 34313236
- PMCID: PMC8289418
- DOI: 10.5152/dir.2021.20813
Diagnostic performance rates of the ACR-TIRADS and EU-TIRADS based on histopathological evidence
Abstract
Purpose: In this study, we aimed to assess the effectiveness of malignancy stratification algorithms of the American College of Radiology (ACR) and European Thyroid Association (ETA) in the delineation of thyroid nodules using a database of nodules that were unequivocally diagnosed by means of histopathological examination and meticulously matched with the imaged nodules.
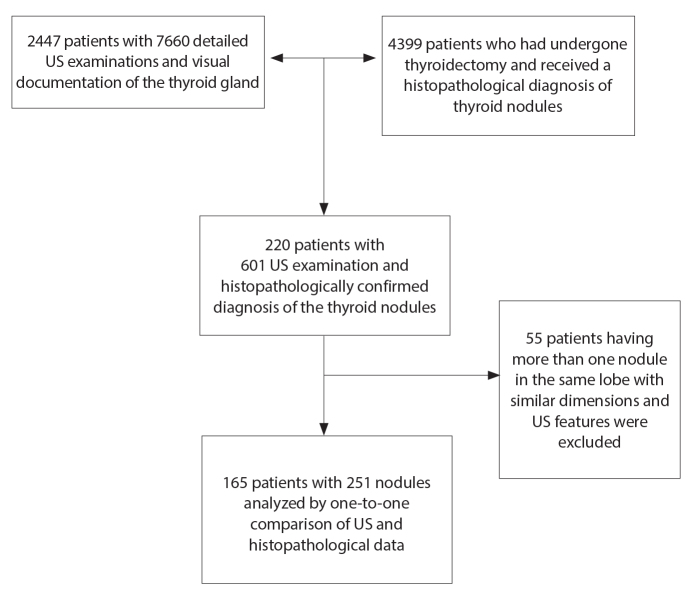
Methods: A total of 165 patients having 251 thyroid nodules with histopathologically proven definitive diagnoses during a 5-year period were included in this study. All patients had preoperatively undergone ultrasonography (US) examination, and US characteristics of the thyroid nodules were retrospectively analyzed and assigned in compliance with the thyroid imaging reporting and data system categories recommended by the ACR (ACR-TIRADS) and ETA (EU-TIRADS). The diagnostic effectiveness in the delineation of thyroid nodules and unnecessary fine-needle aspiration (FNAB) rates were evaluated.
Results: Overall, 189 nodules (75.30%) were diagnosed as benign, while 62 nodules (24.70%) were reported to be malignant based on histopathological assessment. Sensitivity and specificity rates were 71% and 75% for ACR-TIRADS and 73% and 80% for EU-TIRADS. The area under the curve values were 0.78 and 0.80 for ACR-TIRADS and EU-TIRADS, respectively. The unnecessary FNAB rates were 61% for ACR-TIRADS and 64% for EU-TIRADS as per the recommended criteria of each algorithm.
Conclusion: The diagnostic performance of both malignancy stratification systems was signified to be moderate and sufficient in a cohort of nodules with definite histopathological diagnosis. In light of our results, we demonstrated the strengths and weaknesses of the ACR- and EU-TIRADS for physicians who should be familiar with them for optimal management of thyroid nodules.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
