

Post-Acute Sequelae of COVID-19 Pneumonia: Six-month Chest CT Follow-up
- PMID: 34313468
- PMCID: PMC8335814
- DOI: 10.1148/radiol.2021210834
Post-Acute Sequelae of COVID-19 Pneumonia: Six-month Chest CT Follow-up
Abstract
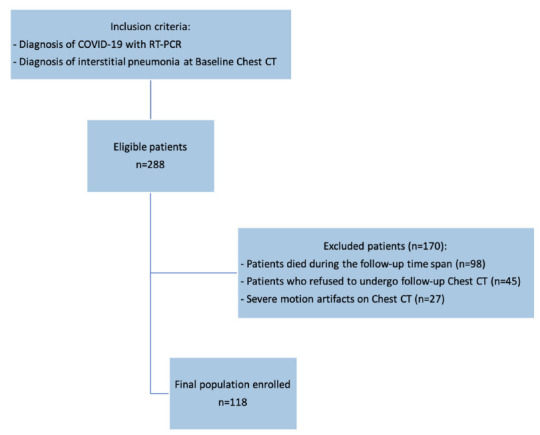
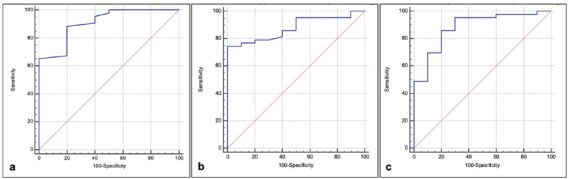
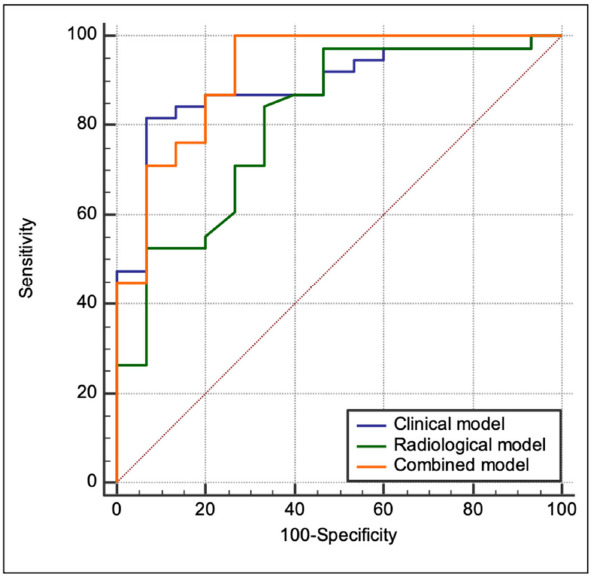
Background The long-term post-acute pulmonary sequelae of COVID-19 remain unknown. Purpose To evaluate lung injury in patients affected by COVID-19 pneumonia at the 6-month follow-up CT examination compared with the baseline chest CT examination. Materials and Methods From March 19, 2020, to May 24, 2020, patients with moderate to severe COVID-19 pneumonia who had undergone baseline chest CT were prospectively enrolled at their 6-month follow-up. The CT qualitative findings, semiquantitative Lung Severity Score (LSS), and the well-aerated lung volume at quantitative chest CT (QCCT) analysis were analyzed. The performance of the baseline LSS and QCCT findings for predicting fibrosis-like changes (reticular pattern and/or honeycombing) at the 6-month follow-up chest CT examination was tested by using receiver operating characteristic curves. Univariable and multivariable logistic regression analyses were used to test clinical and radiologic features that were predictive of fibrosis-like changes. The multivariable analysis was performed with clinical parameters alone (clinical model), radiologic parameters alone (radiologic model), and the combination of clinical and radiologic parameters (combined model). Results One hundred eighteen patients who had undergone baseline chest CT and agreed to undergo follow-up chest CT at 6 months were included in the study (62 women; mean age, 65 years ± 12 [standard deviation]). At follow-up chest CT, 85 of 118 (72%) patients showed fibrosis-like changes and 49 of 118 (42%) showed ground-glass opacities. The baseline LSS (>14) and QCCT findings (≤3.75 L and ≤80%) showed excellent performance for predicting fibrosis-like changes at follow-up chest CT. In the multivariable analysis, the areas under the curve were 0.89 (95% CI: 0.77, 0.96) for the clinical model, 0.81 (95% CI: 0.68, 0.9) for the radiologic model, and 0.92 (95% CI: 0.81, 0.98) for the combined model. Conclusion At 6-month follow-up chest CT, 72% of patients showed late sequelae, in particular fibrosis-like changes. The baseline Lung Severity Score and the well-aerated lung volume at quantitative chest CT (QCCT) analysis showed excellent performance for predicting fibrosis-like changes at the 6-month chest CT (area under the curve, >0.88). Male sex, cough, lymphocytosis, and the well-aerated lung volume at QCCT analysis were significant predictors of fibrosis-like changes at 6 months, demonstrating an inverse correlation (area under the curve, 0.92). © RSNA, 2021 See also the editorial by Wells and Devaraj in this issue.
Figures
Comment in
-
Residual Lung Disease at Six-month Follow-up CT after COVID-19: Clinical Significance Is a Key Issue.Radiology. 2021 Nov;301(2):E406-E408. doi: 10.1148/radiol.2021211284. Epub 2021 Jul 27. Radiology. 2021. PMID: 34313479 Free PMC article. No abstract available.
Comment on
-
Thin-Section Computed Tomography Manifestations During Convalescence and Long-Term Follow-Up of Patients with Severe Acute Respiratory Syndrome (SARS).Med Sci Monit. 2016 Aug 8;22:2793-9. doi: 10.12659/msm.896985. Med Sci Monit. 2016. PMID: 27501327 Free PMC article.
-
Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: a 15-year follow-up from a prospective cohort study.Bone Res. 2020 Feb 14;8:8. doi: 10.1038/s41413-020-0084-5. eCollection 2020. Bone Res. 2020. PMID: 32128276 Free PMC article.
References
-
- Naming the coronavirus disease (COVID-19) and the virus that causes it. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technica.... Published 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
