

Ultrasonographic assessment of the caudal vena cava diameter in cats during blood donation
- PMID: 34313488
- PMCID: PMC9160942
- DOI: 10.1177/1098612X211028838
Ultrasonographic assessment of the caudal vena cava diameter in cats during blood donation
Abstract
Objectives: Ultrasonography of the caudal vena cava (CVC) has been previously established to assess fluid status in dogs but not in cats. The aim of this study was to determine CVC diameter changes during feline blood donation.
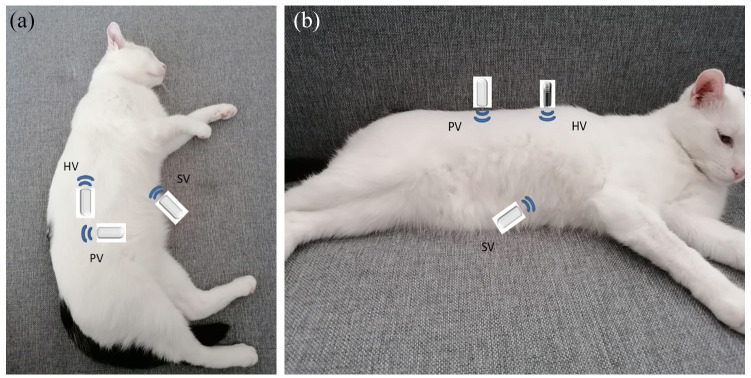
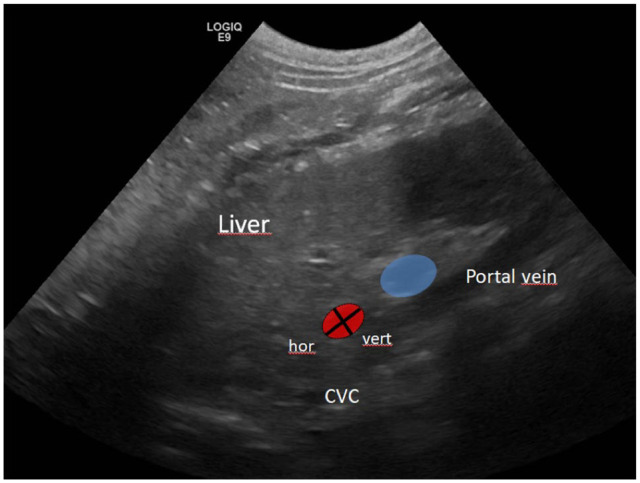
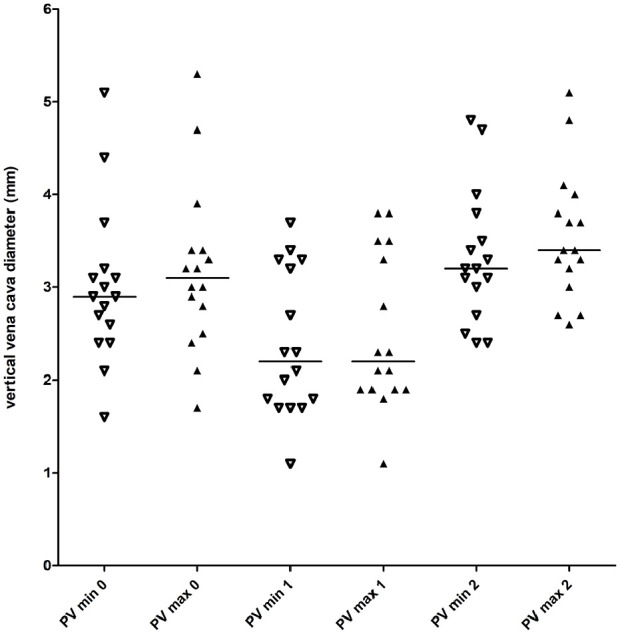
Methods: Inter- and intra-observer variability were assessed in 11 client-owned cats. Minimal and maximal CVC diameters were assessed longitudinally in the subxiphoid view (SV) and right paralumbar view (PV), and transversely in the right hepatic intercostal view (HV). Eighteen client-owned, healthy, anaesthetised cats were evaluated during 21 blood donation procedures of 10 ml/kg in the same anatomical locations before (T0) and after (T1) blood donation, and after volume resuscitation with 30 ml/kg lactated Ringer's solution (T2). The CVC index was calculated.
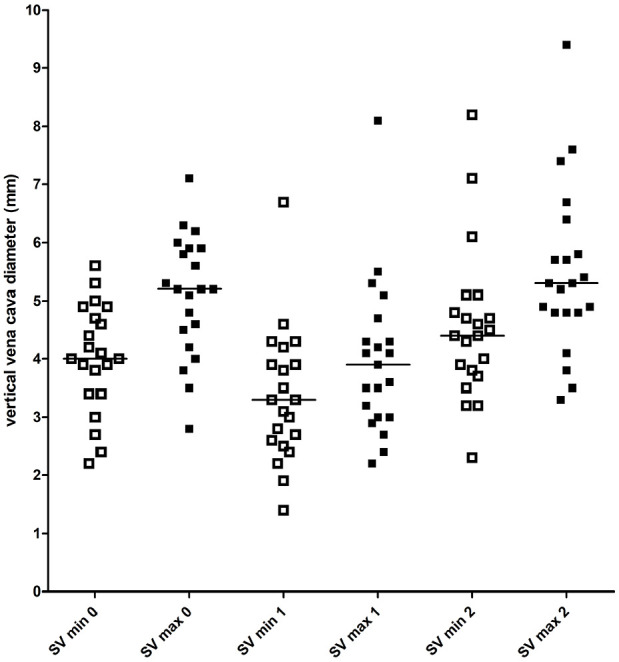
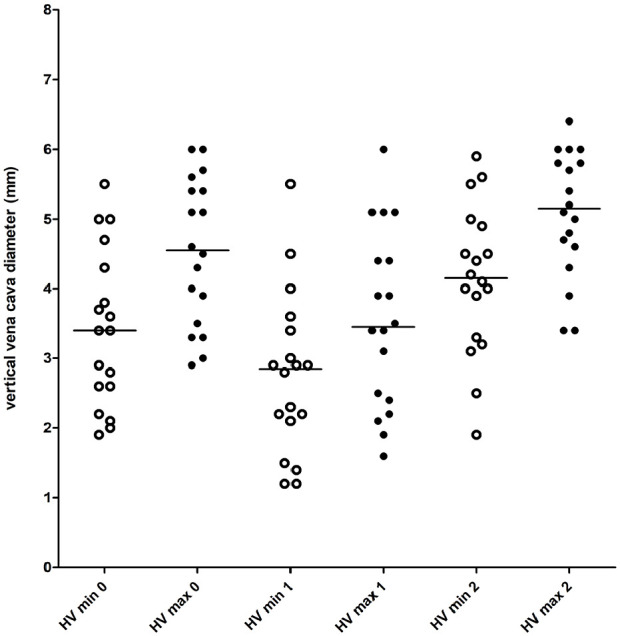
Results: Intra-observer variability was acceptable for all probe positions, except for the HV, whereas inter-observer variability was considered unacceptable for all probe positions. Complete measurements were obtained during 21 blood donations at T0, T1 and T2 at the SV, during 18/21 blood donations at the HV and during 16/21 blood donations at the PV. At the SV, the minimal CVC diameter between T1 and T2 (P <0.001), and the maximal CVC diameter between T0 and T1 and between T1 and T2 (P <0.001) were significantly different. At the HV, the minimal vertical diameter, maximal vertical diameter and minimal horizontal diameter were different between all timepoints (P <0.001). The maximal horizontal diameter was different between T1 and T2 (P = 0.002). At the PV, both diameters were different between all timepoints (P <0.001). The CVC index was not different between timepoints.
Conclusion and relevance: Significant probe position dependent CVC diameter changes with marked overlap were observed before and after blood donation, and after fluid bolus. No absolute CVC diameter could be used to indicate hypovolaemia. Ultrasonographic assessment of the feline CVC is highly operator-dependent. The CVC index is not useful in cats.
Keywords: Point-of-care ultrasound; hypovolaemia; intravascular volume status; vena cava index.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Davis H, Jensen T, Johnson A, et al. 2013 AAHA/AAFP fluid therapy guidelines for dogs and cats. J Am Anim Hosp Assoc 2013; 49: 149–159. - PubMed
-
- Marik PE. Techniques for assessment of intravascular volume in critically ill patients. J Intensive Care Med 2009; 24: 329–337. - PubMed
-
- Wilson M, Davis DP, Coimbra R. Diagnosis and monitoring of hemorrhagic shock during the initial resuscitation of multiple trauma patients: a review. J Emerg Med 2003; 24: 413–422. - PubMed
-
- Celebi Yamanoglu NG, Yamanoglu A, Parlak I, et al. The role of inferior vena cava diameter in volume status monitoring; the best sonographic measurement method? Am J Emerg Med 2015; 33: 433–438. - PubMed
-
- Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest 2008; 134: 172–178. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
