

Supracondylar fractures in children: management and treatment
- PMID: 34313666
- PMCID: PMC8420822
- DOI: 10.23750/abm.v92iS3.11725
Supracondylar fractures in children: management and treatment
Abstract
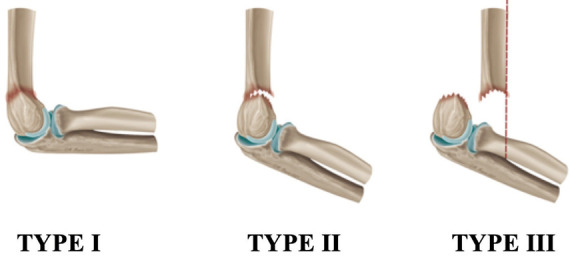
Supracondylar humeral fractures are widely considered the most common elbow fracture in children. Gartland classification plays a fundamental role in decision-making regarding management and prognosis. Recent literature recommends conservative management for non or minimally displaced fractures, whereas there seems to be a trend towards surgical treatment for all displaced fractures. The preferred treatment for displaced Gartland II and Gartland III fractures is closed reduction and percutaneous fixation with lateral pins. In particular patterns medial pin is recommended for obtain a stable construct. Neurovascular complications are mostly associated with Type III fractures and sometimes surgical exploration with fracture reduction is needed. Correct diagnosis and proper management protocol is mandatory for avoid early and late complications such as neurovascular impairment and malunion.
Conflict of interest statement
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article.
Figures
References
-
- Otsuka NY, Kasser JR. Supracondylar fractures of the humerus in children. J Am Acad Orthop Surg. 1997;5:19–26. doi: 10.5435/00124635-199701000-00003. - PubMed
-
- Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J Pediatr Orthop B. 2001;10:63–67. PMID: 1126981. - PubMed
-
- Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. J Pediatr Orthop. 1998;18:38–42. PMID 9449099. - PubMed
-
- Villarin LA, Belk KE, Freid R. Emergency department evaluation and treatment of elbow and forearm injuries. Emerg Med Clin North Am. 1999;17(4):843–58. PMID: 10584105 DOI: 10.1016/s0733-8627(05)70100-0. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
