

Effect of 7 vs 14 Days of Antibiotic Therapy on Resolution of Symptoms Among Afebrile Men With Urinary Tract Infection: A Randomized Clinical Trial
- PMID: 34313686
- PMCID: PMC8317010
- DOI: 10.1001/jama.2021.9899
Effect of 7 vs 14 Days of Antibiotic Therapy on Resolution of Symptoms Among Afebrile Men With Urinary Tract Infection: A Randomized Clinical Trial
Abstract
Importance: Determination of optimal treatment durations for common infectious diseases is an important strategy to preserve antibiotic effectiveness.
Objective: To determine whether 7 days of treatment is noninferior to 14 days when using ciprofloxacin or trimethoprim/sulfamethoxazole to treat urinary tract infection (UTI) in afebrile men.
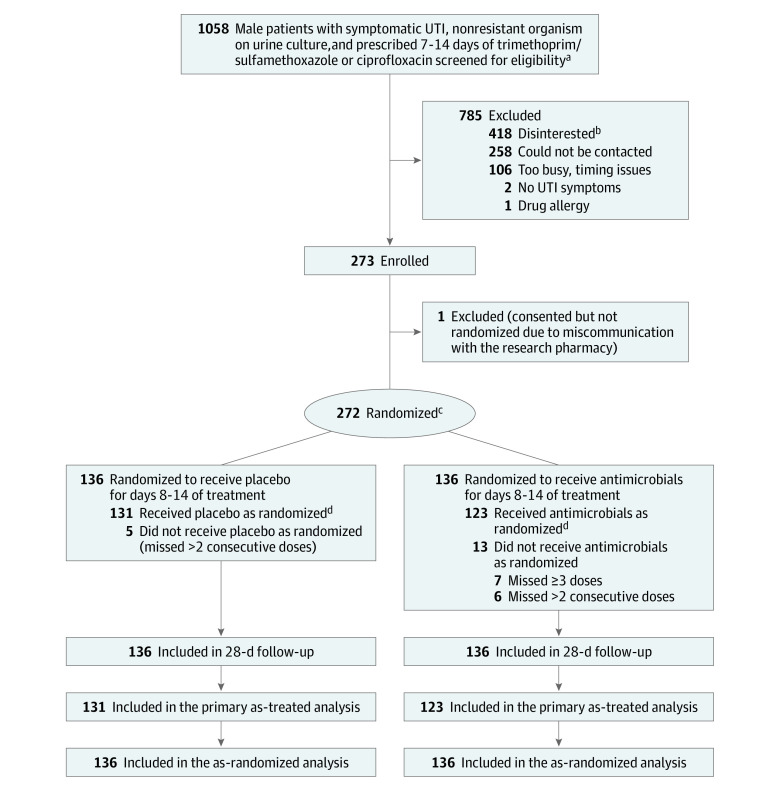
Design, setting, and participants: Randomized, double-blind, placebo-controlled noninferiority trial of afebrile men with presumed symptomatic UTI treated with ciprofloxacin or trimethoprim/sulfamethoxazole at 2 US Veterans Affairs medical centers (enrollment, April 2014 through December 2019; final follow-up, January 28, 2020). Of 1058 eligible men, 272 were randomized.
Interventions: Participants continued the antibiotic prescribed by their treating clinician for 7 days of treatment and were randomized to receive continued antibiotic therapy (n = 136) or placebo (n = 136) for days 8 to 14 of treatment.
Main outcomes and measures: The prespecified primary outcome was resolution of UTI symptoms by 14 days after completion of active antibiotic treatment. A noninferiority margin of 10% was selected. The as-treated population (participants who took ≥26 of 28 doses and missed no more than 2 consecutive doses) was used for the primary analysis, and a secondary analysis included all patients as randomized, regardless of treatment adherence. Secondary outcomes included recurrence of UTI symptoms and/or adverse events within 28 days of stopping study medication.
Results: Among 272 patients (median [interquartile range] age, 69 [62-73] years) who were randomized, 100% completed the trial and 254 (93.4%) were included in the primary as-treated analysis. Symptom resolution occurred in 122/131 (93.1%) participants in the 7-day group vs 111/123 (90.2%) in the 14-day group (difference, 2.9% [1-sided 97.5% CI, -5.2% to ∞]), meeting the noninferiority criterion. In the secondary as-randomized analysis, symptom resolution occurred in 125/136 (91.9%) participants in the 7-day group vs 123/136 (90.4%) in the 14-day group (difference, 1.5% [1-sided 97.5% CI, -5.8% to ∞]) Recurrence of UTI symptoms occurred in 13/131 (9.9%) participants in the 7-day group vs 15/123 (12.9%) in the 14-day group (difference, -3.0% [95% CI, -10.8% to 6.2%]; P = .70). Adverse events occurred in 28/136 (20.6%) participants in the 7-day group vs 33/136 (24.3%) in the 14-day group.
Conclusions and relevance: Among afebrile men with suspected UTI, treatment with ciprofloxacin or trimethoprim/sulfamethoxazole for 7 days was noninferior to 14 days of treatment with regard to resolution of UTI symptoms by 14 days after antibiotic therapy. The findings support the use of a 7-day course of ciprofloxacin or trimethoprim/sulfamethoxazole as an alternative to a 14-day course for treatment of afebrile men with UTI.
Trial registration: ClinicalTrials.gov identifier: NCT01994538.
Conflict of interest statement
Figures
Comment in
-
Shorter Courses of Antibiotics for Urinary Tract Infection in Men.JAMA. 2021 Jul 27;326(4):309-310. doi: 10.1001/jama.2021.11120. JAMA. 2021. PMID: 34313705 No abstract available.
-
Benign Prostatic Hyperplasia.J Urol. 2022 Jan;207(1):201-204. doi: 10.1097/JU.0000000000002275. Epub 2021 Oct 18. J Urol. 2022. PMID: 34661444 No abstract available.
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2022 Feb;207(2):456-458. doi: 10.1097/JU.0000000000002321. Epub 2021 Nov 17. J Urol. 2022. PMID: 34784725 No abstract available.
-
Effect of 7 vs 14 Days of Antibiotics Among Afebrile Men With Urinary Tract Infection.JAMA. 2021 Nov 23;326(20):2079-2080. doi: 10.1001/jama.2021.16741. JAMA. 2021. PMID: 34812872 No abstract available.
-
Effect of 7 vs 14 Days of Antibiotics Among Afebrile Men With Urinary Tract Infection.JAMA. 2021 Nov 23;326(20):2080. doi: 10.1001/jama.2021.16738. JAMA. 2021. PMID: 34812873 No abstract available.
-
Effect of 7 vs 14 Days of Antibiotics Among Afebrile Men With Urinary Tract Infection.JAMA. 2021 Nov 23;326(20):2079. doi: 10.1001/jama.2021.16735. JAMA. 2021. PMID: 34812874 No abstract available.
-
In afebrile men with UTIs, 7 d of ciprofloxacin or trimethoprim-sulfamethoxazole was noninferior to 14 d.Ann Intern Med. 2021 Dec;174(12):JC141. doi: 10.7326/ACPJ202112210-141. Epub 2021 Dec 7. Ann Intern Med. 2021. PMID: 34871046
-
Infection and Inflammation of Genitourinary Tract.J Urol. 2022 May;207(5):1132-1133. doi: 10.1097/JU.0000000000002463. Epub 2022 Feb 10. J Urol. 2022. PMID: 35139652 No abstract available.
-
Seven Versus 14 Days of Antibiotic Therapy for Men With Afebrile Urinary Tract Infections: Is a Longer Course Really Stronger in Men?Ann Emerg Med. 2022 Nov;80(5):471-473. doi: 10.1016/j.annemergmed.2022.09.017. Ann Emerg Med. 2022. PMID: 36265924 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
