

Cost-effectiveness of Dapagliflozin for the Treatment of Heart Failure With Reduced Ejection Fraction
- PMID: 34313742
- PMCID: PMC8317009
- DOI: 10.1001/jamanetworkopen.2021.14501
Cost-effectiveness of Dapagliflozin for the Treatment of Heart Failure With Reduced Ejection Fraction
Abstract
Importance: Heart failure with reduced ejection fraction produces substantial morbidity, mortality, and health care costs. Dapagliflozin is the first sodium-glucose cotransporter 2 inhibitor approved for the treatment of heart failure with reduced ejection fraction.
Objective: To examine the cost-effectiveness of adding dapagliflozin to guideline-directed medical therapy for heart failure with reduced ejection fraction in patients with or without diabetes.
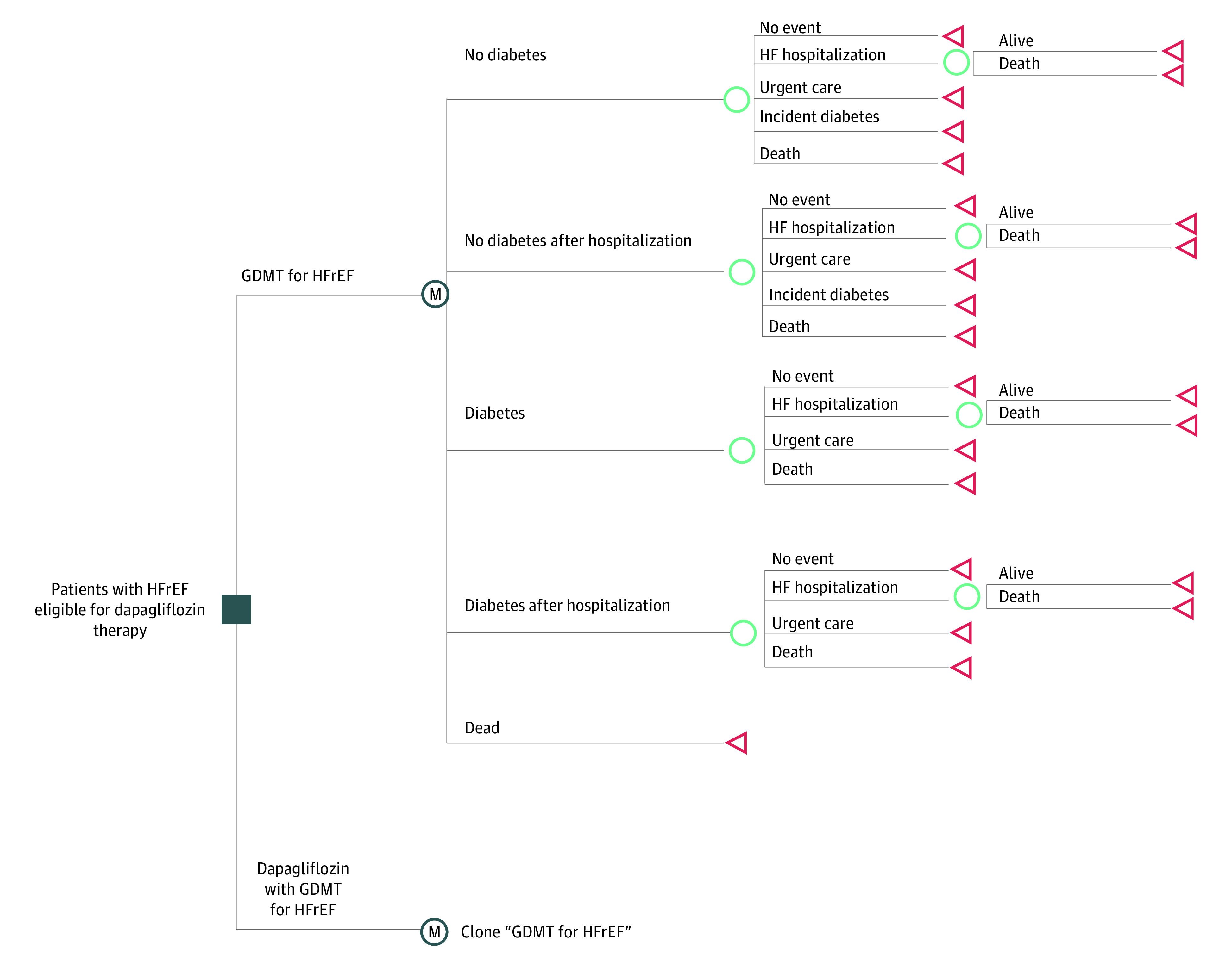
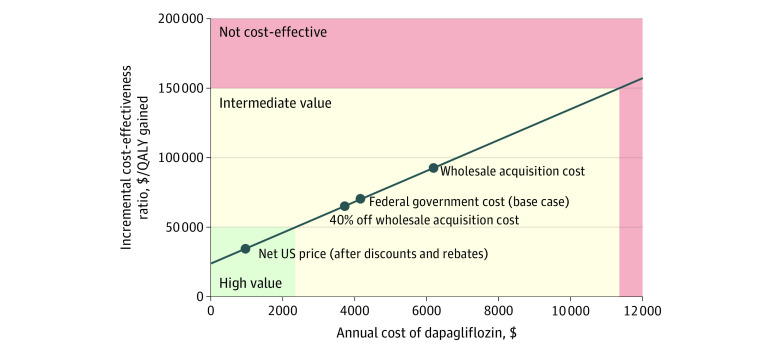
Design, setting, and participants: This economic evaluation developed and used a Markov cohort model that compared dapagliflozin and guideline-directed medical therapy with guideline-directed medical therapy alone in a hypothetical cohort of US adults with similar clinical characteristics as participants of the Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction (DAPA-HF) trial. Dapagliflozin was assumed to cost $4192 annually. Nonparametric modeling was used to estimate long-term survival. Deterministic and probabilistic sensitivity analyses examined the impact of parameter uncertainty. Data were analyzed between September 2019 and January 2021.
Main outcomes and measures: Lifetime incremental cost-effectiveness ratio in 2020 US dollars per quality-adjusted life-year (QALY) gained.
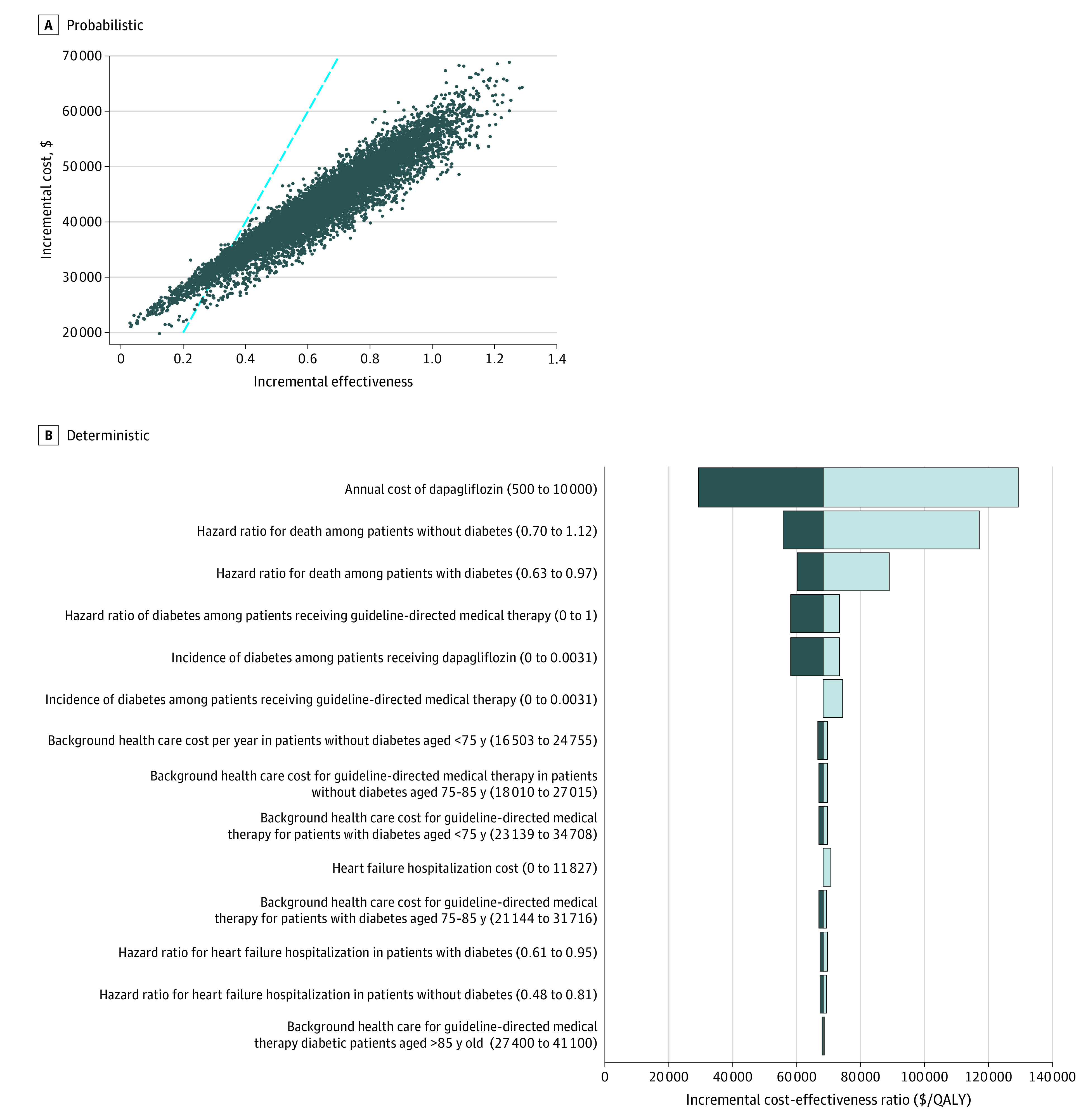
Results: The simulated cohort had a starting age of 66 years, and 41.8% had diabetes at baseline. Median (interquartile range) survival in the guideline-directed medical therapy arm was 6.8 (3.5-11.3) years. Dapagliflozin was projected to add 0.63 (95% uncertainty interval [UI], 0.25-1.15) QALYs at an incremental lifetime cost of $42 800 (95% UI, $37 100-$50 300), for an incremental cost-effectiveness ratio of $68 300 per QALY gained (95% UI, $54 600-$117 600 per QALY gained; cost-effective in 94% of probabilistic simulations at a threshold of $100 000 per QALY gained). Findings were similar in individuals with or without diabetes but were sensitive to drug cost.
Conclusions and relevance: In this study, adding dapagliflozin to guideline-directed medical therapy was projected to improve long-term clinical outcomes in patients with heart failure with reduced ejection fraction and be cost-effective at current US prices. Scalable strategies for improving uptake of dapagliflozin may improve long-term outcomes in patients with heart failure with reduced ejection fraction.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
