

Assessing the impact of medically tailored meals and medical nutrition therapy on type 2 diabetes: Protocol for Project MiNT
- PMID: 34314856
- PMCID: PMC8453110
- DOI: 10.1016/j.cct.2021.106511
Assessing the impact of medically tailored meals and medical nutrition therapy on type 2 diabetes: Protocol for Project MiNT
Abstract
Background: Research has shown that among people with type 2 diabetes mellitus, reduction in hemoglobin A1c (HbA1c) prevents long term complications. Medically tailored meals (MTM) and telehealth-delivered medical nutrition therapy (tele-MNT) are promising strategies for patient-centered diabetes care.
Objectives: Project MiNT will determine whether provision of MTM with and without the addition of telehealth-delivered medical nutrition therapy improves HbA1c and is cost effective for patients with type 2 diabetes mellitus.
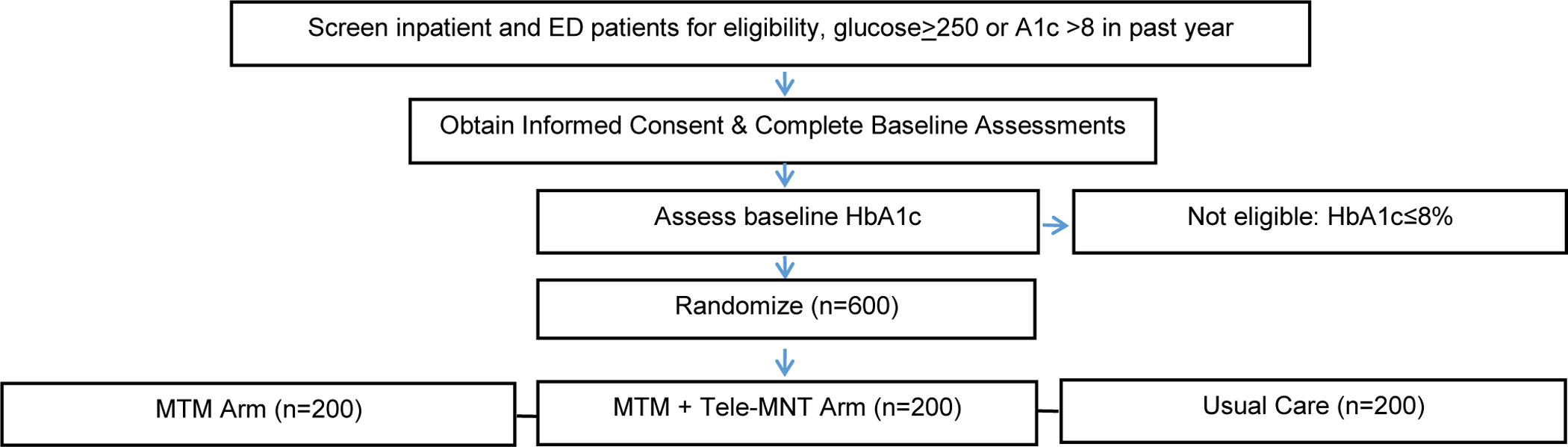
Methods: Patients with poorly controlled type 2 diabetes mellitus (HbA1c >8%) will be recruited from Jefferson Health. Eligible patients will be randomized to one of three arms: 1) usual care, 2) 12 weeks of home-delivered MTM, or 3) MTM + 12 months of tele-MNT. All participants (n = 600) will complete three follow-up assessments at 3, 6, and 12 months. The primary outcome is change in HbA1c at 6 months. Secondary outcomes include change in HbA1c at 3 and 12 months and cost-effectiveness of the intervention at 6 and 12 months. Conclusion Findings from Project MiNT will inform MTM coverage and financing decisions, how to structure services for scalability and system-wide integration, and the role of these services in reducing health disparities.
Keywords: Diabetes mellitus; Hemoglobin A1c; Medical nutrition therapy; Medically tailored meals; Telehealth.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest
The authors have no competing interests to disclose.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Schiller J, Lucas J, Peregoy J, Summary Health Statistics for U.S. Population: National Health Interview Survey, 2011. National Center for Health Statistics., Vital Heal. Stat 10 (2012). - PubMed
-
- DHHS, National Diabetes Statistics Report, 2020, Natl. Diabetes Stat. Rep (2020) 2. - PubMed
-
- AHRQ, Diabetes Disparities Among Racial and Ethnic Minorities, Agency Healthc. Res. Qual (2001) 1–6.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
