

Multi-Institutional Practice-Patterns in Fetal Congenital Heart Disease Following Implementation of a Standardized Clinical Assessment and Management Plan
- PMID: 34315235
- PMCID: PMC8475692
- DOI: 10.1161/JAHA.121.021598
Multi-Institutional Practice-Patterns in Fetal Congenital Heart Disease Following Implementation of a Standardized Clinical Assessment and Management Plan
Abstract
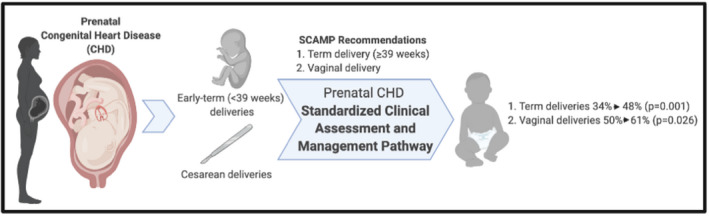
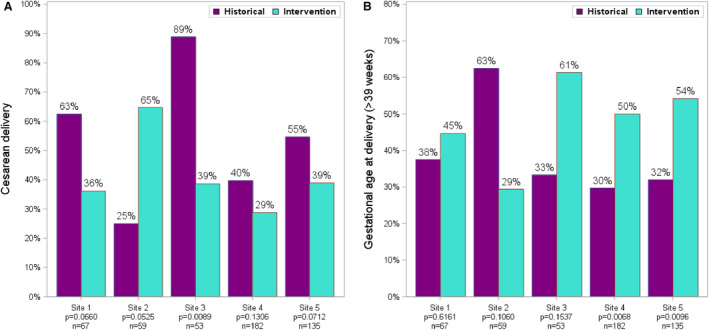
Background Prenatal diagnosis of congenital heart disease has been associated with early-term delivery and cesarean delivery (CD). We implemented a multi-institutional standardized clinical assessment and management plan (SCAMP) through the University of California Fetal-Maternal Consortium. Our objective was to decrease early-term (37-39 weeks) delivery and CD in pregnancies complicated by fetal congenital heart disease using a SCAMP methodology to improve practice in a high-risk and clinically complex setting. Methods and Results University of California Fetal-Maternal Consortium site-specific management decisions were queried following SCAMP implementation. This contemporary intervention group was compared with a University of California Fetal-Maternal Consortium historical cohort. Primary outcomes were early-term delivery and CD. A total of 496 maternal-fetal dyads with prenatally diagnosed congenital heart disease were identified, 185 and 311 in the historical and intervention cohorts, respectively. Recommendation for later delivery resulted in a later gestational age at delivery (38.9 versus 38.1 weeks, P=0.01). After adjusting for maternal age and site, historical controls were more likely to have a CD (odds ratio [OR],1.8; 95% CI, 2.1-2.8; P=0.004) and more likely (OR, 2.1; 95% CI, 1.4-3.3) to have an early-term delivery than the intervention group. Vaginal delivery was recommended in 77% of the cohort, resulting in 61% vaginal deliveries versus 50% in the control cohort (P=0.03). Among pregnancies with major cardiac lesions (n=373), vaginal birth increased from 51% to 64% (P=0.008) and deliveries ≥39 weeks increased from 33% to 48% (P=0.004). Conclusions Implementation of a SCAMP decreased the rate of early-term deliveries and CD for prenatal congenital heart disease. Development of clinical pathways may help standardize care, decrease maternal risk secondary to CD, improve neonatal outcomes, and reduce healthcare costs.
Keywords: SCAMP; cesarean; fetal CHD; obstetrics; prenatal congenital heart disease.
Conflict of interest statement
None.
Figures
References
-
- Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D, Goffinet F. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983–2000: a population‐based evaluation. Pediatrics. 2005;115:95–101. DOI: 10.1542/peds.2004-0516. - DOI - PubMed
