

Virus Induced Lymphocytes (VIL) as a novel viral antigen-specific T cell therapy for COVID-19 and potential future pandemics
- PMID: 34315945
- PMCID: PMC8316478
- DOI: 10.1038/s41598-021-94654-y
Virus Induced Lymphocytes (VIL) as a novel viral antigen-specific T cell therapy for COVID-19 and potential future pandemics
Abstract
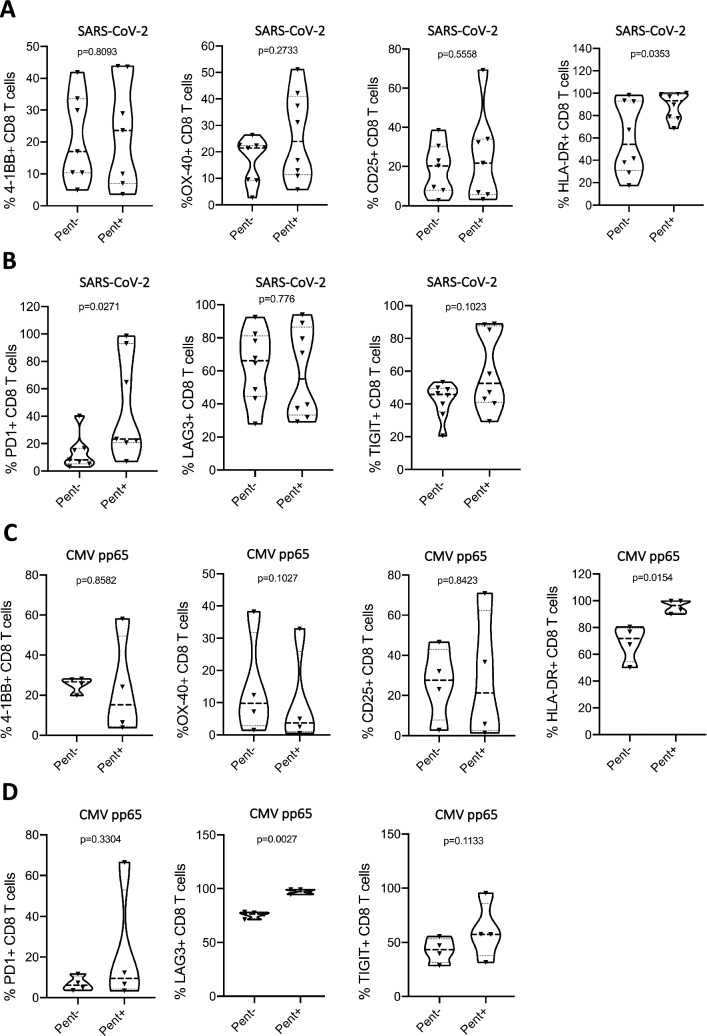
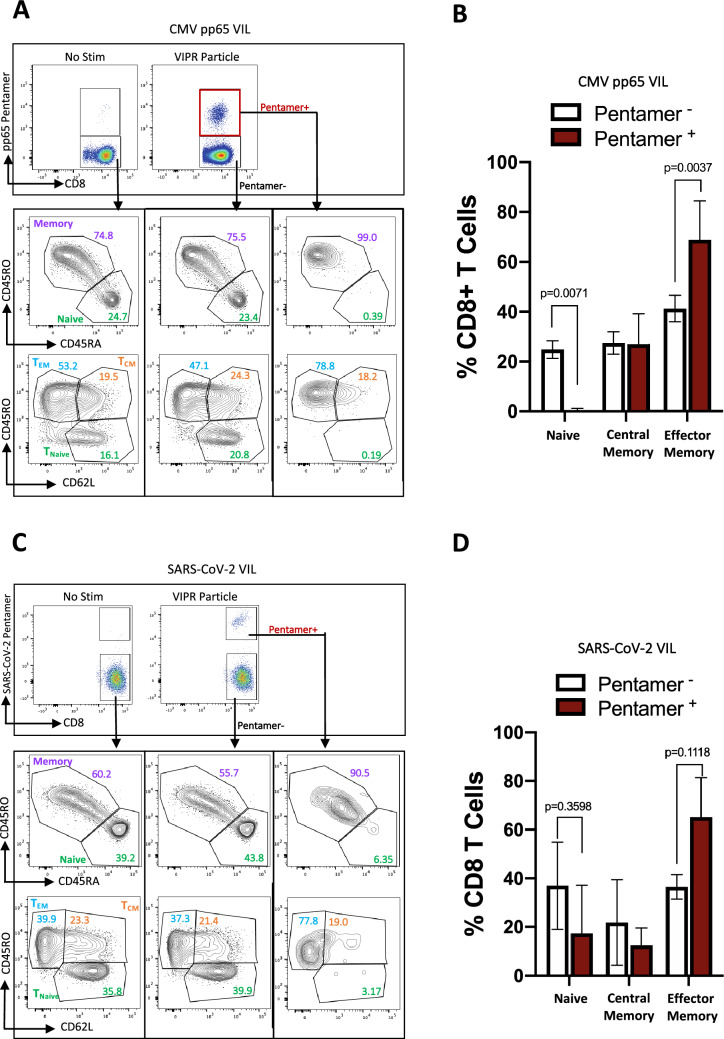
The a priori T cell repertoire and immune response against SARS-CoV-2 viral antigens may explain the varying clinical course and prognosis of patients having a mild COVID-19 infection as opposed to those developing more fulminant multisystem organ failure and associated mortality. Using a novel SARS-Cov-2-specific artificial antigen presenting cell (aAPC), coupled with a rapid expansion protocol (REP) as practiced in tumor infiltrating lymphocytes (TIL) therapy, we generate an immune catalytic quantity of Virus Induced Lymphocytes (VIL). Using T cell receptor (TCR)-specific aAPCs carrying co-stimulatory molecules and major histocompatibility complex (MHC) class-I immunodominant SARS-CoV-2 peptide-pentamer complexes, we expand virus-specific VIL derived from peripheral blood mononuclear cells (PBMC) of convalescent COVID-19 patients up to 1000-fold. This is achieved in a clinically relevant 7-day vein-to-vein time-course as a potential adoptive cell therapy (ACT) for COVID-19. We also evaluate this approach for other viral pathogens using Cytomegalovirus (CMV)-specific VIL from donors as a control. Rapidly expanded VIL are enriched in virus antigen-specificity and show an activated, polyfunctional cytokine profile and T effector memory phenotype which may contribute to a robust immune response. Virus-specific T cells can also be delivered allogeneically via MHC-typing and patient human leukocyte antigen (HLA)-matching to provide pragmatic treatment in a large-scale therapeutic setting. These data suggest that VIL may represent a novel therapeutic option that warrants further clinical investigation in the armamentarium against COVID-19 and other possible future pandemics.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
Off-the-Shelf Partial HLA Matching SARS-CoV-2 Antigen Specific T Cell Therapy: A New Possibility for COVID-19 Treatment.Front Immunol. 2021 Dec 23;12:751869. doi: 10.3389/fimmu.2021.751869. eCollection 2021. Front Immunol. 2021. PMID: 35003063 Free PMC article.
-
Virus-Specific T Cells From Cryopreserved Blood During an Emergent Virus Outbreak for a Potential Off-the-Shelf Therapy.Transplant Cell Ther. 2023 Sep;29(9):572.e1-572.e13. doi: 10.1016/j.jtct.2023.06.001. Epub 2023 Jun 6. Transplant Cell Ther. 2023. PMID: 37290691
-
SARS-CoV-2-specific T cells generated for adoptive immunotherapy are capable of recognizing multiple SARS-CoV-2 variants.PLoS Pathog. 2022 Feb 14;18(2):e1010339. doi: 10.1371/journal.ppat.1010339. eCollection 2022 Feb. PLoS Pathog. 2022. PMID: 35157735 Free PMC article.
-
The role of T-cell-mediated mechanisms in virus infections of the nervous system.Curr Top Microbiol Immunol. 2001;253:219-45. doi: 10.1007/978-3-662-10356-2_11. Curr Top Microbiol Immunol. 2001. PMID: 11417137 Review.
-
Refining human T-cell immunotherapy of cytomegalovirus disease: a mouse model with 'humanized' antigen presentation as a new preclinical study tool.Med Microbiol Immunol. 2016 Dec;205(6):549-561. doi: 10.1007/s00430-016-0471-0. Epub 2016 Aug 18. Med Microbiol Immunol. 2016. PMID: 27539576 Review.
Cited by
-
Effective virus-specific T-cell therapy for high-risk SARS-CoV-2 infections in hematopoietic stem cell transplant recipients: initial case studies and literature review.Geroscience. 2024 Feb;46(1):1083-1106. doi: 10.1007/s11357-023-00858-7. Epub 2023 Jul 6. Geroscience. 2024. PMID: 37414968 Free PMC article. Review.
-
Allogeneic, off-the-shelf, SARS-CoV-2-specific T cells (ALVR109) for the treatment of COVID-19 in high-risk patients.Haematologica. 2023 Jul 1;108(7):1840-1850. doi: 10.3324/haematol.2022.281946. Haematologica. 2023. PMID: 36373249 Free PMC article. Clinical Trial.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
