

Demystifying Sacral Masses: A Pictorial Review
- PMID: 34316126
- PMCID: PMC8299490
- DOI: 10.1055/s-0041-1729766
Demystifying Sacral Masses: A Pictorial Review
Abstract
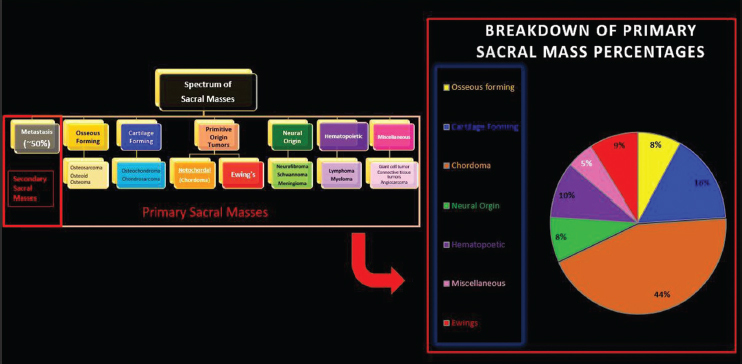
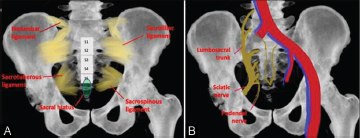
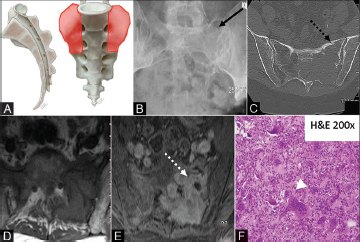
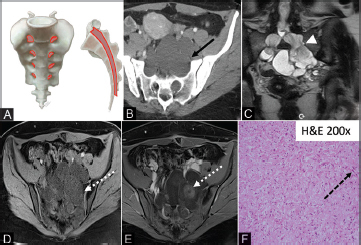
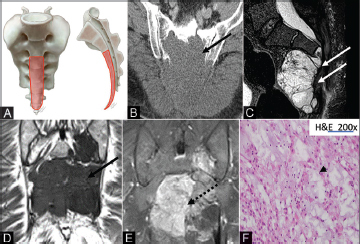
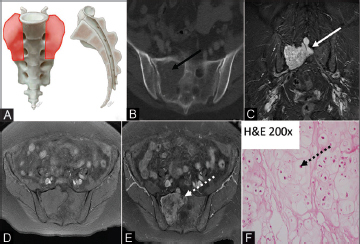
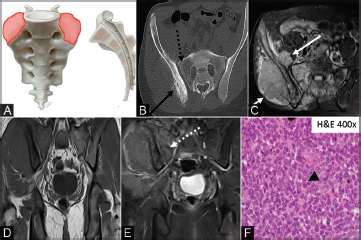
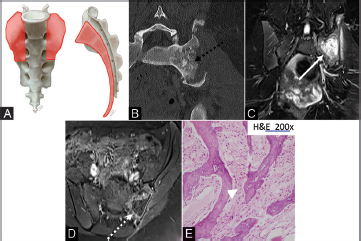
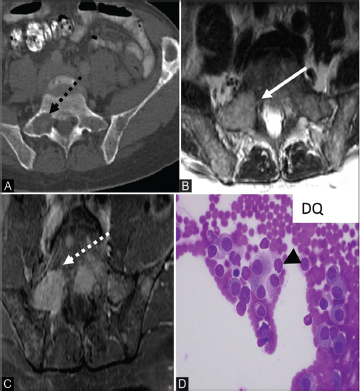
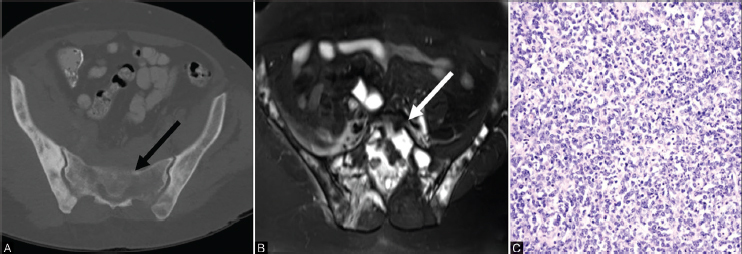
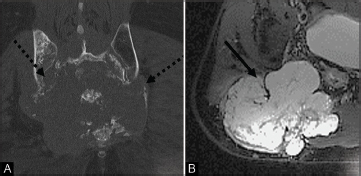
The sacrum is a triangular shaped bone made up of five fused vertebral bodies. It is composed of bone, cartilage, marrow elements as well as notochord remnants and is a common site for both benign and malignant (primary and secondary) tumors. Familiarity with the imaging features and clinical presentations of sacral bone tumors could be helpful in narrowing the differential diagnosis. Magnetic resonance imaging and computed tomography are the preferred imaging modalities for evaluating sacral masses. This pictorial review will highlight imaging features of common sacral tumors with pathologic correlation. Additionally, this article will review some critical principles and helpful tips to successfully biopsy these lesions.
Keywords: chondrosarcoma; chordoma; giant cell tumor; metastasis; osteosarcoma; sacrum.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflicts of InterestFinancial Support and Sponsorship There are no conflicts of interest. Nil.
Figures
References
-
- Junming M, Cheng Y, Dong C et al.Giant cell tumor of the cervical spine: a series of 22 cases and outcomes. Spine. 2008;33(03):280–288. - PubMed
-
- Llauger J, Palmer J, Amores S, Bagué S, Camins A. Primary tumors of the sacrum: diagnostic imaging. AJR Am J Roentgenol. 2000;174(02):417–424. - PubMed
-
- Varga P P, Bors I, Lazary A. Sacral tumors and management. Orthop Clin North Am. 2009;40(01):105–123, vii. - PubMed
-
- Disler D G, Miklic D. Imaging findings in tumors of the sacrum. AJR Am J Roentgenol. 1999;173(06):1699–1706. - PubMed
LinkOut - more resources
Full Text Sources