

A Rare Case of Severe Nontropical Isolated Right Ventricular Endomyocardial Fibrosis
- PMID: 34317112
- PMCID: PMC8299774
- DOI: 10.1016/j.jaccas.2020.09.042
A Rare Case of Severe Nontropical Isolated Right Ventricular Endomyocardial Fibrosis
Abstract
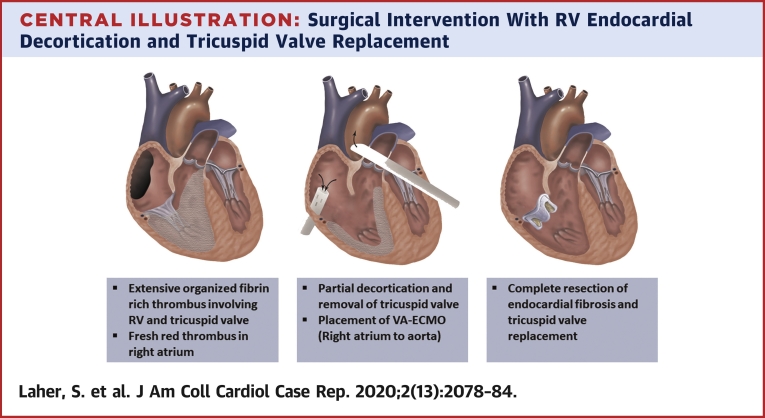
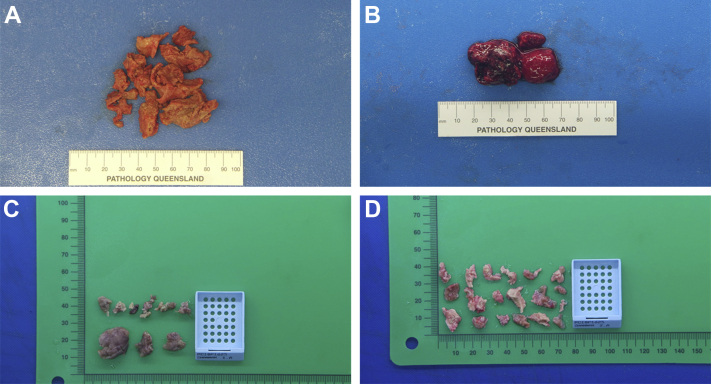
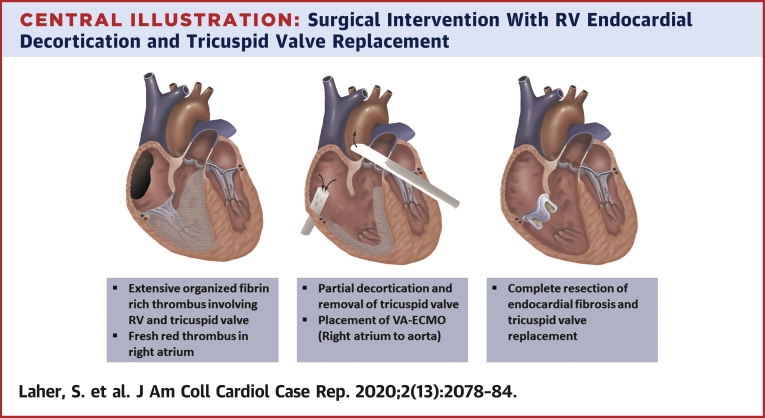
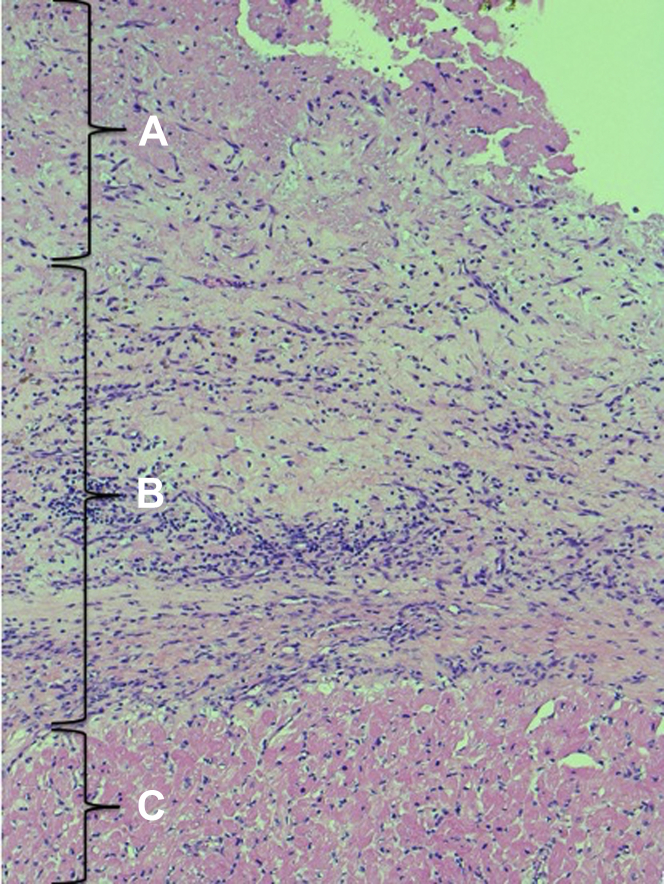
We present a case of late presentation nontropical endomyocardial fibrosis isolated to the right ventricle and tricuspid valve (TV). In response to deteriorating hemodynamics, surgical debulking and TV removal were performed before initiation of centralized venoarterial extracorporeal membrane oxygenation support. Definitive endomyocardial resection with a TV prosthesis was then successfully completed. (Level of Difficulty: Advanced.).
Keywords: CE, contrast-enhanced; CMR, cardiac magnetic resonance; ECMO, extracorporeal membrane oxygenation; EMF, endomyocardial fibrosis; LV, left ventricular; RA, right atrial; RV, right ventricular; RVOT, right ventricular outflow tract; TTE, Transthoracic echocardiogram; TV, tricuspid valve; contrast enhanced TTE; endomyocardial fibrosis; right ventricle.
Crown Copyright © 2020 Published by Elsevier on behalf of the American College of Cardiology Foundation.
Conflict of interest statement
Dr. Platts is acting as a medical liaison for Lantheus Medical Imaging. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Grimaldi A., Mocumbi A.O., Freers J. Tropical endomyocardial fibrosis: natural history, challenges, and perspectives. Circulation. 2016;133:2503–2515. - PubMed
-
- Mankad R., Bonnichsen C., Mankad S. Hypereosinophilic syndrome: cardiac diagnosis and management. Heart. 2016;102:100–106. - PubMed
-
- Mocumbi A.O., Ferreira M.B., Sidi D., Yacoub M.H. A population study of endomyocardial fibrosis in a rural area of Mozambique. N Engl J Med. 2008;359:43–49. - PubMed
-
- Moraes F., Lapa C., Hazin S., Tenorio E., Gomes C., Moraes C.R. Surgery for endomyocardial fibrosis revisited. Eur J Cardiothorac Surg. 1999;15:309–312. discussion 312–3. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
