

An Uncommon Cause of ST-Segment Elevation Myocardial Infarction: Intramural Coronary Artery Hematoma After Blunt Chest Trauma
- PMID: 34317160
- PMCID: PMC8304548
- DOI: 10.1016/j.jaccas.2020.09.032
An Uncommon Cause of ST-Segment Elevation Myocardial Infarction: Intramural Coronary Artery Hematoma After Blunt Chest Trauma
Abstract
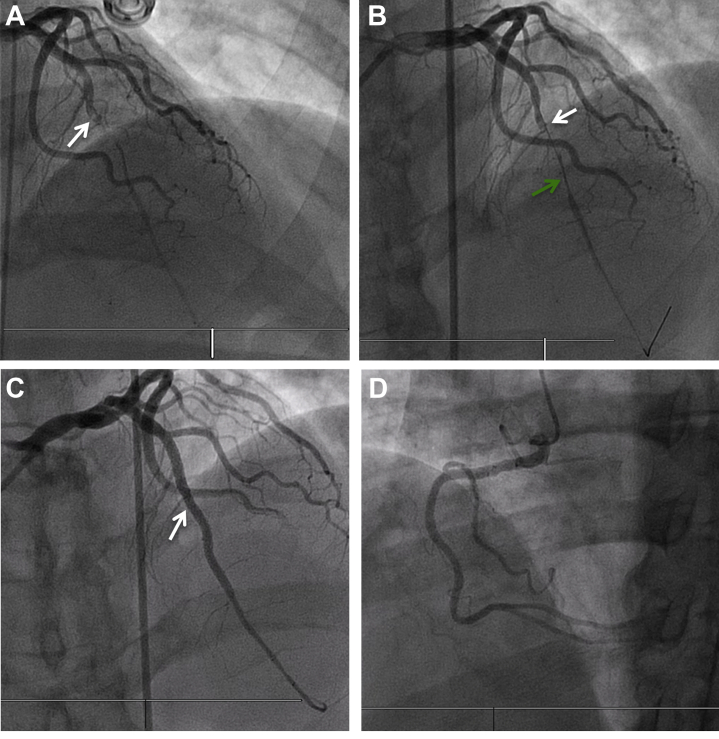
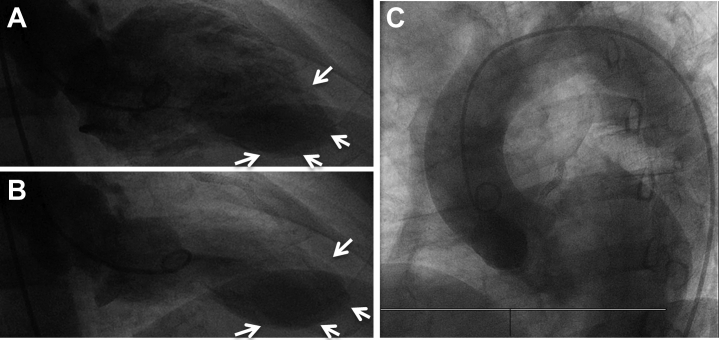
Intramural coronary hematoma (IMCH) is a rare cause of acute myocardial infarction (MI). We aim to review the current knowledge and share our experience with the diagnosis and management of a patient presenting with traumatic IMCH leading to an acute ST-segment elevation MI. (Level of Difficulty: Intermediate.).
Keywords: BCT, blunt chest trauma; CP, chest pain; DAPT, dual anti-platelet therapy; ECG, electrocardiogram; IMCH, intramural coronary hematoma; IVUS, intravascular ultrasound; LAD, left anterior descending artery; MI, myocardial infarction; PCI, percutaneous coronary intervention; SCAD, spontaneous coronary artery dissection; STEMI, ST segment elevation myocardial infarction; TIMI, Thrombolysis In Myocardial Infarction; acute coronary syndrome; chest pain; dissection; intravascular ultrasound; myocardial infarction; percutaneous coronary intervention.
© 2020 The Authors.
Conflict of interest statement
This material is the result of work supported with resources and the use of facilities at the Veterans Affairs, Caribbean Healthcare System San Juan, P.R. The contents of this publication do not represent the views of the Veterans Affairs Caribbean Healthcare System, the U.S. Department of Veterans Affairs, or the United States Government. All authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures





References
-
- Shenoda M. Aragon J. Coronary intramural hematomas: a focused review. Interv Cardiol. 2015;7:239–249.
-
- Christensen M.D., Nielsen P.E., Sleight P. Prior blunt chest trauma may be a cause of single vessel coronary disease; hypothesis and review. Int J Cardiol. 2006;108:1–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
