

Associations between oxygen delivery and cardiac index with hyperlactatemia during cardiopulmonary bypass
- PMID: 34317766
- PMCID: PMC8299069
- DOI: 10.1016/j.xjtc.2020.04.001
Associations between oxygen delivery and cardiac index with hyperlactatemia during cardiopulmonary bypass
Abstract
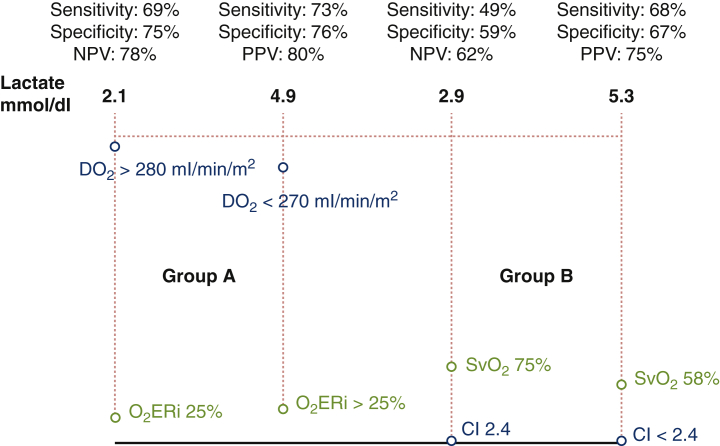
Objective: Metabolism management plays an essential role during cardiopulmonary bypass (CPB). There are different metabolic management devices integrated to heart-lung machines; the most commonly used and accepted metabolic target is indexed oxygen delivery (DO2i) (280 mL/min/m2) and cardiac index (CI) (2.4 L/min/m2), which can be managed independently or according to other metabolic parameters. Our objective was to compare lactate production during CPB procedures using different metabolic management: DO2i in relation to indexed oxygen extraction ratio (O2ERi) and CI in relation to mixed venous oxygen saturation (SvO2).
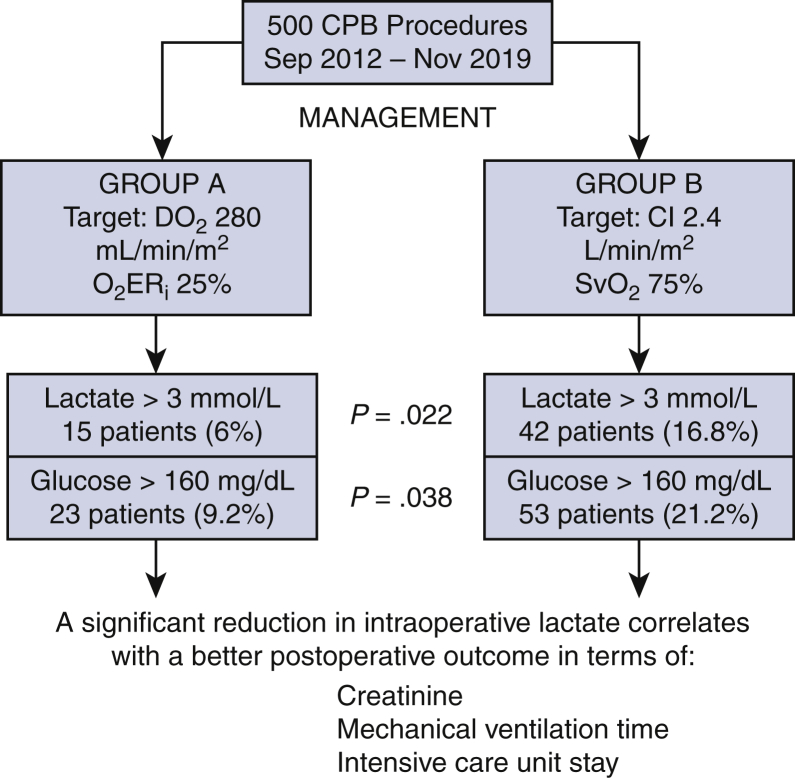
Methods: Data on 500 CPB procedures were retrospectively collected in a specialized regional tertiary cardiac surgery center in Italy between September and 2012 and November 2019. In group A, the DO2i with 280 mL/min/m2 target in relation to O2ERi 25% was used; in group B, CI with 2.4 L/min/m2 target in relation to SvO2 75% was used. During CPB, serial arterial blood gas analyses with blood lactate and glucose determinations were obtained. Hyperlactatemia (HL) was defined as a peak arterial blood lactate concentration >3 mmol/L. The postoperative outcome of patients with or without HL was compared.
Results: Eight pre- and intraoperative factors were found to be significantly associated with peak blood lactate level during CPB at univariate analysis. HL (>3 mmol/L) was detected in 15 (6%) patients of group A and in 42 (16.8%) patients of group B (P = .022); hyperglycemia (>160 mg/dL) was found in 23 (9.2%) patients of group A and in 53 (21.2%) patients of group B (P = .038). Patients with HL during CPB had a significant increase in serum creatinine value, higher rate of prolonged mechanical ventilation time and intensive care unit stay. A cutoff of DO2i <270 mL/min/m2 in relation to O2ERi >35% in group A and a cutoff of CI <2.4 L/min/m2 in relation to SvO2 <65% in group B were found to have a positive predictive value of 80% and 75% for HL, respectively. A cutoff of DO2i >290 mL/min/m2 in relation to O2ERi 24% in group A and a cutoff of CI >2.4 L/min/m2 in relation to SvO2 >75% in group B were found to have a negative predictive value of 78% and 62% for HL, respectively.
Conclusions: This retrospective observational analysis showed that management of DO2i in relation to O2ERi was 16% more specific in terms of negative predictive value for HL during CPB compared with the use of CI in relation to SvO2. Group A reported a significant reduction in the incidence of intraoperative lactate peak, correlated with postoperative reduction of serum creatinine value, mechanical ventilation time, and intensive care unit stay, compared with group B.
Keywords: CI, cardiac index; CPB, cardiopulmonary bypass; DO2i, indexed oxygen delivery; HL, hyperlactatemia; Hb, hemoglobin; Hct, hematocrit; ICU, intensive care unit; O2ERi, indexed oxygen extraction ratio; SvO2, venous oxygen saturation; cardiac index; cardiopulmonary bypass; hyperlactatemia; oxygen delivery.
© 2020 The Authors.
Figures






References
-
- Demers P., Elkouri S., Martineau R., Couturier A., Cartier R. Outcome with high blood lactate levels during cardiopulmonary bypass in adult cardiac surgery. Ann Thorac Surg. 2000;70:2082–2086. - PubMed
-
- Ranucci M., Isgrò G., Romitti F., Mele S., Biagioli B., Giomarelli P. Anaerobic metabolism during cardiopulmonary bypass: the predictive value of carbon dioxide derived parameters. Ann Thorac Surg. 2006;81:2189–2195. - PubMed
-
- Maillet J.M., Le Besnerais P., Cantoni M., Nataf P., Ruffenach A., Lessana A., et al. Frequency, risk factors, and outcome of hyperlactatemia after cardiac surgery. Chest. 2003;123:1361–1366. - PubMed
-
- Landow L. Splanchnic lactate production in cardiac surgery patients. Crit Care Med. 1993;21(2 suppl):S84–S91. - PubMed
-
- Boldt J., Piper S., Murray P., Lehmann A. Case 2-1999. Severe lactic acidosis after cardiac surgery: sign of perfusion deficits. J Cardiothorac Vasc Anesth. 1999;13:220–224. - PubMed
LinkOut - more resources
Full Text Sources
