

Endovascular exclusion of the entire aortic arch with branched stent-grafts after surgery for acute type A aortic dissection
- PMID: 34317796
- PMCID: PMC8302916
- DOI: 10.1016/j.xjtc.2020.04.009
Endovascular exclusion of the entire aortic arch with branched stent-grafts after surgery for acute type A aortic dissection
Abstract
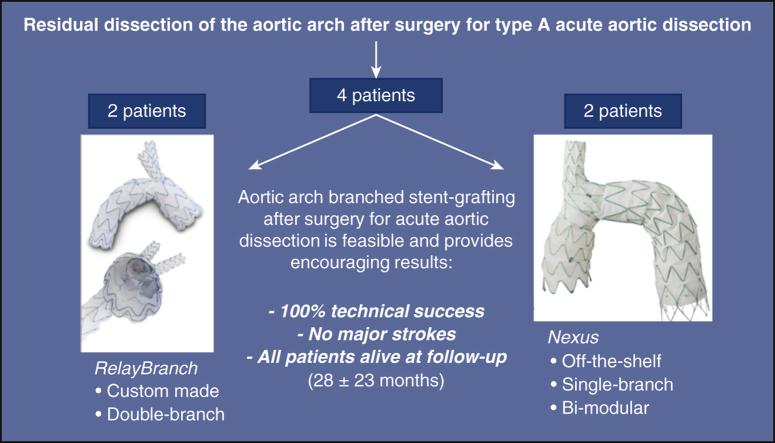
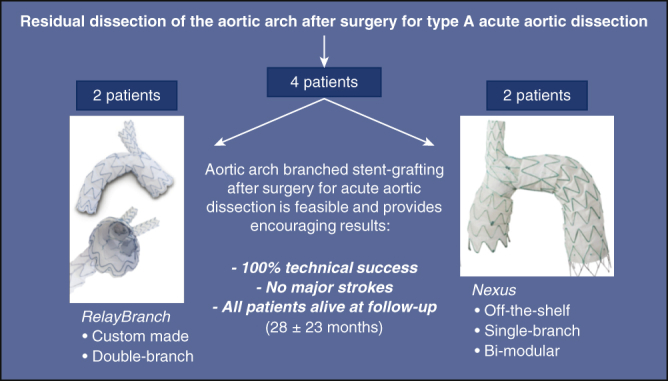
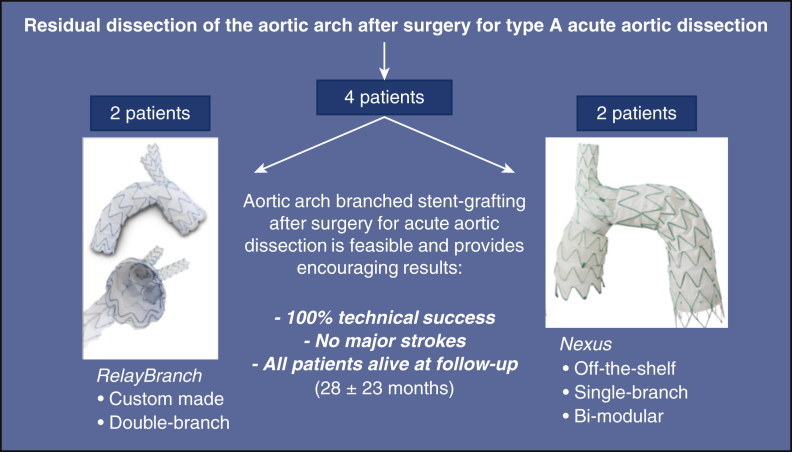
Background: The treatment of residual pathology of the aortic arch after surgical repair for type A acute dissection (AAD) represents a therapeutic challenge. Recently, new branched endovascular devices have expanded the possibility of aortic arch stent-grafting (ASG) with proximal landing in zone 0. The aim of this retrospective, single-center study was to evaluate outcomes of patients with a history of surgical repair for AAD undergoing ASG with branched devices.
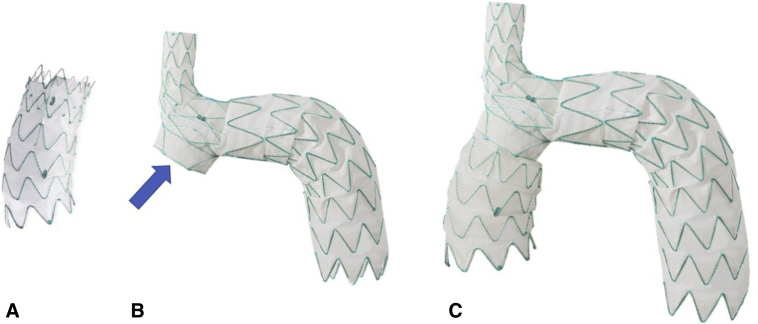
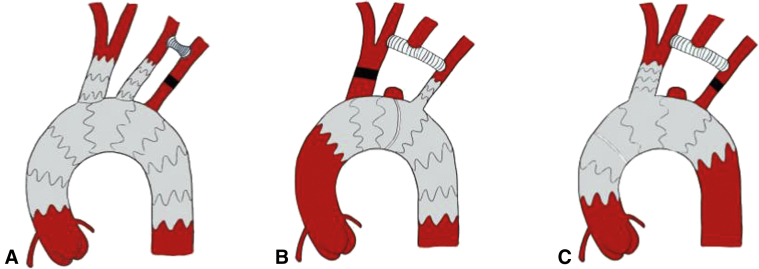
Methods: We analyzed patients undergoing ASG after treatment for type AAD with 2 different branched devices: Nexus (dual-module, single branch, off-the-shelf) and RelayBranch (single-module, dual branch, custom-made). Before ASG, surgical bypass of supra-aortic vessels was performed according to patient's anatomy and to the selected device. All patients underwent clinical and computed tomography scan evaluation before hospital discharge, at 6 months, and on a yearly basis thereafter.
Results: From March 2017 to April 2019, 4 consecutive patients underwent ASG after surgery for AAD at our institution. Mean time from surgery for AAD to ASG was 20 months. Mean age at the time of ASG was 72 years. Nexus and Relay were implanted in 2 patients each. All patients survived and were successfully discharged. Mean intensive care unit stay and hospital stay were 3 and 19 days, respectively. We did not observe any major adverse events. At a mean follow-up of 28 months, all patients are alive and computed tomography scans showed good anatomic results with no endoleaks.
Conclusions: This preliminary experience shows that ASG after surgery for AAD is feasible and provides encouraging clinical and anatomic early results.
Keywords: AAD, type A acute aortic dissection; ASG, aortic arch stent-grafting; BCT, brachiocephalic trunk; CT, computed tomography; LCCA, left common carotid artery; LSA, left subclavian artery; RCCA, right common carotid artery; aortic arch; endovascular therapy.
© 2020 The Authors.
Figures

References
-
- Rylski B., Hahn N., Beyersdorf F., Kondov S., Wolkewitz M., Blanke P., et al. Fate of the dissected aortic arch after ascending replacement in type A aortic dissection. Eur J Cardiothorac Surg. 2017;51:1127–1134. - PubMed
-
- Martens A., Beckmann E., Kaufeld T., Umminger J., Fleissner F., Koigeldiyev N., et al. Total aortic arch repair: risk factor analysis and follow-up in 199 patients. Eur J Cardiothorac Surg. 2016;50:940–948. - PubMed
-
- Spear R., Haulon S., Ohki T., Tsilimparis N., Kanaoka Y., Milne C.P., et al. Subsequent results for arch aneurysm repair with inner branched endografts. Eur J Vasc Endovasc Surg. 2016;51:380–385. - PubMed
-
- D'Onofrio A., Gerosa G. Technique versus technology and the (r)evolution of cardiac surgery: a professional journey from classical surgery to embracing intervention. Eur J Cardiothorac Surg. 2017;52:835–837. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
