

Scimitar syndrome: A new multipatch technique and incidence of postoperative pulmonary vein obstruction
- PMID: 34318016
- PMCID: PMC8303092
- DOI: 10.1016/j.xjtc.2020.07.027
Scimitar syndrome: A new multipatch technique and incidence of postoperative pulmonary vein obstruction
Abstract
Objective: A review of our center's experience before March 2011 showed that one half of 36 patients who had a baffling or reimplantation procedure to repair scimitar syndrome developed pulmonary vein obstruction. We analyzed the results of a new operation that enlarges the left atrium and avoids circuitous pathways or tension on the scimitar pulmonary vein.
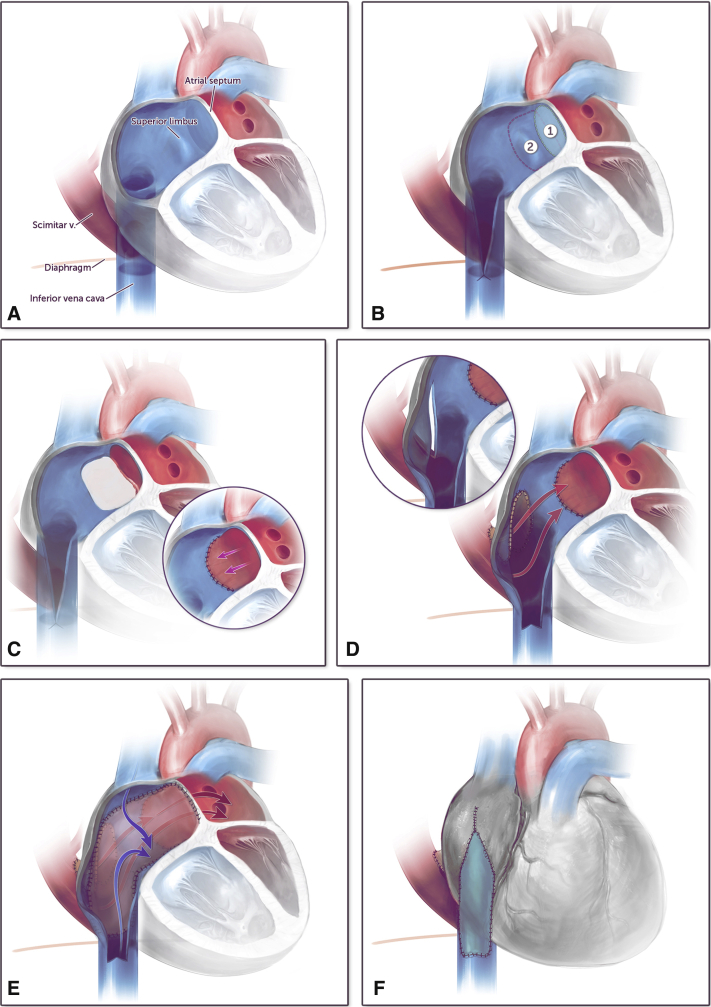
Methods: Between April 2011 and November 2018, 22 patients underwent scimitar vein surgery; 11 had baffling or reimplantation and 11 only had the new operation that included resection of the atrial septum with removal of the muscular limbus. The left atrium was pulled down toward the scimitar vein and a V-shaped incision made at the scimitar vein atrial junction with the space filled with a pulmonary homograft. If the scimitar vein coursed adjacent to the atrium, a V-shaped incision was made into the scimitar vein and directly anastomosed to the atrium. A patch of autologous pericardium was used to septate the atrium and an additional patch placed anteriorly to augment the inferior vena cava.
Results: Of the 11 patients who had baffling or reimplantation, 5 developed pulmonary vein obstruction between 45 days and 9.5 months after surgery associated with baffle thrombosis or tension on the pulmonary vein. None of the 11 patients who only had the new procedure developed pulmonary vein obstruction during postoperative monitoring up to 3.6 years.
Conclusions: Patients having only the multipatch procedure for repair of scimitar syndrome have not developed postoperative pulmonary vein obstruction in the short to intermediate term.
Keywords: CMR, cardiac magnetic resonance; IVC, inferior vena cava; congenital heart disease; partial anomalous pulmonary venous return; pulmonary vein stenosis; scimitar syndrome.
© 2020 The Authors.
Figures






References
-
- Neill C.A., Ferencz C., Sabiston D.C., Sheldon H. The familial occurrence of hypoplastic right lung with systemic arterial supply and venous drainage “scimitar syndrome.”. Bull Johns Hopkins Hosp. 1960;107:1–15. - PubMed
-
- Najm H.K., Williams W.G., Coles J.G., Rebeyka I.M., Freedom R.M. Scimitar syndrome: twenty years' experience and results of repair. J Thorac Cardiovasc Surg. 1996;112:1161–1169. - PubMed
-
- Canter C.E., Martin T.C., Spray T.L., Weldon C.S., Strauss A.W. Scimitar syndrome in childhood. Am J Cardiol. 1986;58:652–654. - PubMed
-
- Dupuis C., Charaf L.A.C., Brevière G.M., Abou P. “Infantile” form of the scimitar syndrome with pulmonary hypertension. Am J Cardiol. 1993;71:1326–1330. - PubMed
-
- Dupuis C., Charaf L.A.C., Brevière G.M., Abou P., Rémy-Jardin M., Helmius G. The “adult” form of the scimitar syndrome. Am J Cardiol. 1992;70:502–507. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
