

Reimplantation valve-sparing aortic root replacement is the most durable approach to facilitate aortic valve repair
- PMID: 34318210
- PMCID: PMC8311546
- DOI: 10.1016/j.xjtc.2020.12.042
Reimplantation valve-sparing aortic root replacement is the most durable approach to facilitate aortic valve repair
Abstract
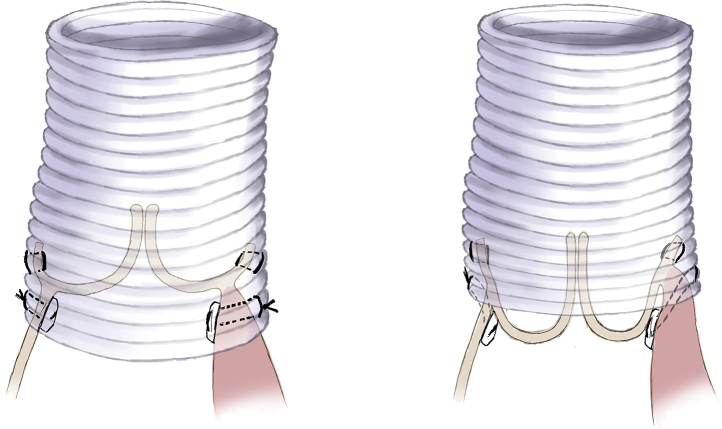
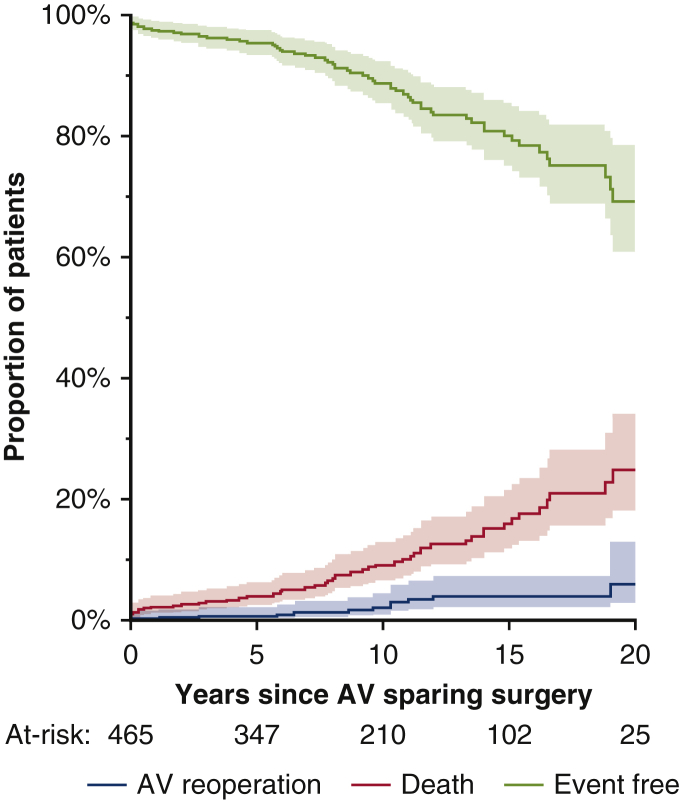
Reimplantation of the aortic valve has been performed for 3 decades, and experience shows that patient selection and meticulous operative technique are crucial to provide excellent clinical outcomes and stable aortic valve function for decades. More than the type of the Dacron graft used for the reimplantation (straight graft or Valsalva graft), we believe that attention to certain technical aspects of this operation is key to a successful and durable aortic valve reconstruction. This article describes the operative procedure as we believe it should be performed based on a learned experience with several hundred cases and summarizes the latest outcomes in a large cohort of patients followed prospectively during the past 3 decades.
Keywords: David operation; aortic insufficiency; aortic root aneurysm; aortic valve; aortic valve repair.
© 2021 The Authors.
Figures








Comment in
-
New horizons in aortic valve repair.JTCVS Tech. 2021 Apr 26;7:71. doi: 10.1016/j.xjtc.2021.04.018. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34471910 Free PMC article. No abstract available.
References
-
- David T.E., Feindel C.M. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg. 1992;103:617–622. - PubMed
-
- David T.E. Remodeling of the aortic root and preservation of the native aortic valve. Op Tech Cardiac Thorac Surg. 1996;1:44–56.
-
- David T.E. Aortic valve sparing in different aortic valve and aortic root conditions. J Am Coll Cardiol. 2016;68:654–664. - PubMed
-
- Schneider U., Aicher D., Miura H., Schäfers H.J. Suture annuloplasty in aortic valve repair. Ann Thorac Surg. 2016;101:783–785. - PubMed
-
- Lansac E., Di Centa I., Sleilaty G., Lejeune S., Berrebi A., Zacek P., et al. Remodeling root repair with an external aortic ring annuloplasty. J Thorac Cardiovasc Surg. 2017;153:1033–1042. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
