

The role of diffuse correlation spectroscopy and frequency-domain near-infrared spectroscopy in monitoring cerebral hemodynamics during hypothermic circulatory arrests
- PMID: 34318236
- PMCID: PMC8311503
- DOI: 10.1016/j.xjtc.2021.01.023
The role of diffuse correlation spectroscopy and frequency-domain near-infrared spectroscopy in monitoring cerebral hemodynamics during hypothermic circulatory arrests
Abstract
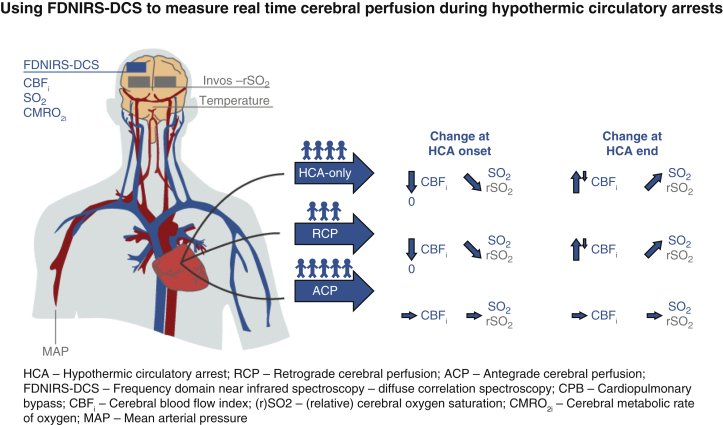
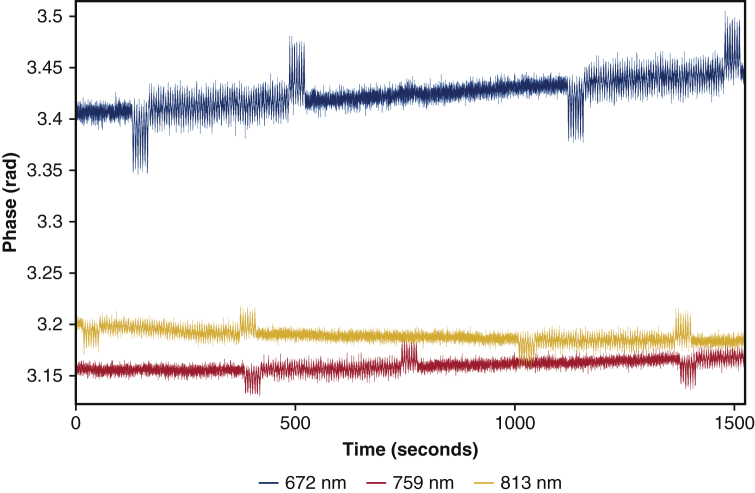
Objectives: Real-time noninvasive monitoring of cerebral blood flow (CBF) during surgery is key to reducing mortality rates associated with adult cardiac surgeries requiring hypothermic circulatory arrest (HCA). We explored a method to monitor cerebral blood flow during different brain protection techniques using diffuse correlation spectroscopy (DCS), a noninvasive optical technique which, combined with frequency-domain near-infrared spectroscopy (FDNIRS), also provides a measure of oxygen metabolism.
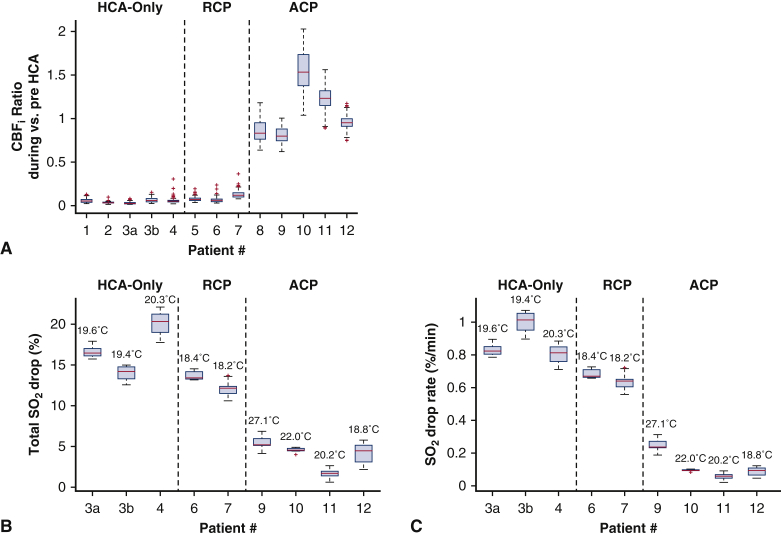
Methods: We used DCS in combination with FDNIRS to simultaneously measure hemoglobin oxygen saturation (SO2), an index of cerebral blood flow (CBFi), and an index of cerebral metabolic rate of oxygen (CMRO2i) in 12 patients undergoing cardiac surgery with HCA.
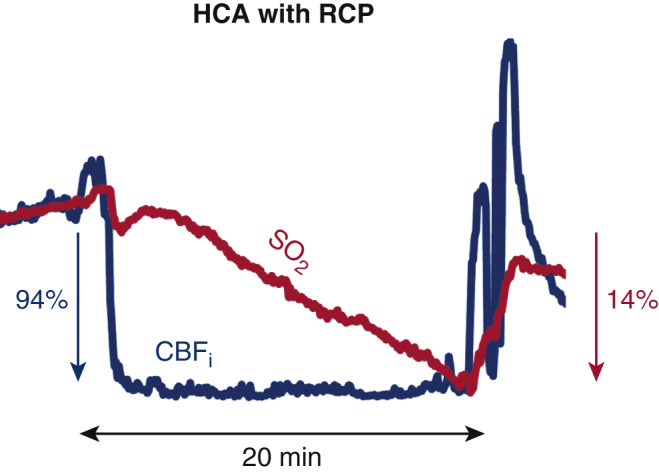
Results: Our measurements revealed that a negligible amount of blood is delivered to the cerebral cortex during HCA with retrograde cerebral perfusion, indistinguishable from HCA-only cases (median CBFi drops of 93% and 95%, respectively) with consequent similar decreases in SO2 (mean decrease of 0.6 ± 0.1% and 0.9 ± 0.2% per minute, respectively); CBFi and SO2 are mostly maintained with antegrade cerebral perfusion; the relationship of CMRO2i to temperature is given by CMRO2i = 0.052e0.079T.
Conclusions: FDNIRS-DCS is able to detect changes in CBFi, SO2, and CMRO2i with intervention and can become a valuable tool for optimizing cerebral protection during HCA.
Keywords: ACP, antegrade cerebral perfusion; CBFi, cerebral blood flow (index); CMRO2i, cerebral metabolic rate of oxygen (index); CPB, cardiopulmonary bypass; DCS, diffuse correlation spectroscopy; EEG, electroencephalography; FDNIRS, frequency-domain near-infrared spectroscopy; HCA, hypothermic circulatory arrest; NIRS, near-infrared spectroscopy; RCP, retrograde cerebral perfusion; SO2, hemoglobin oxygen saturation; TCD, transcranial Doppler ultrasound; antegrade cerebral perfusion; brain imaging; cerebral blood flow; diffuse correlation spectroscopy; hypothermic circulatory arrest; near-infrared spectroscopy; rSO2, regional oxygen saturation; retrograde cerebral perfusion.
© 2021 The Authors.
Figures







References
-
- Mezrow C.K., Sadeghi A.M., Gandsas A., Dapunt O.E., Shiang H.H., Zappulla R.A., et al. Cerebral effects of low-flow cardiopulmonary bypass and hypothermic circulatory arrest. Ann Thorac Surg. 1994;57:532–539. - PubMed
-
- Wypij D., Newburger J.W., Rappaport L.A., duPlessis A.J., Jonas R.A., Wernovsky G., et al. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: the Boston circulatory arrest trial. J Thorac Cardiovasc Surg. 2003;126:1397–1403. - PubMed
-
- Gaynor J.W., Nicolson S.C., Jarvik G.P., Wernovsky G., Montenegro L.M., Burnham N.B., et al. Increasing duration of deep hypothermic circulatory arrest is associated with an increased incidence of postoperative electroencephalographic seizures. J Thorac Cardiovasc Surg. 2005;130:1278–1286. - PMC - PubMed
-
- Czerny M., Fleck T., Zimpfer D., Dworschak M., Hofmann W., Hutschala D., et al. Risk factors of mortality and permanent neurologic injury in patients undergoing ascending aortic and arch repair. J Thorac Cardiovasc Surg. 2003;126:1296–1301. - PubMed
-
- Englum B.R., He X., Gulack B.C., Ganapathi A.M., Mathew J.P., Brennan J.M., et al. Hypothermia and cerebral protection strategies in aortic arch surgery: a comparative effectiveness analysis from the STS adult cardiac surgery database. Eur J Cardiothorac Surg. 2017;52:492–498. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
