

Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine
- PMID: 34318288
- PMCID: PMC8299287
- DOI: 10.1016/j.lanepe.2021.100178
Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine
Abstract
Background: Dialysis and kidney transplant patients are vulnerable populations for COVID-19 related disease and mortality.
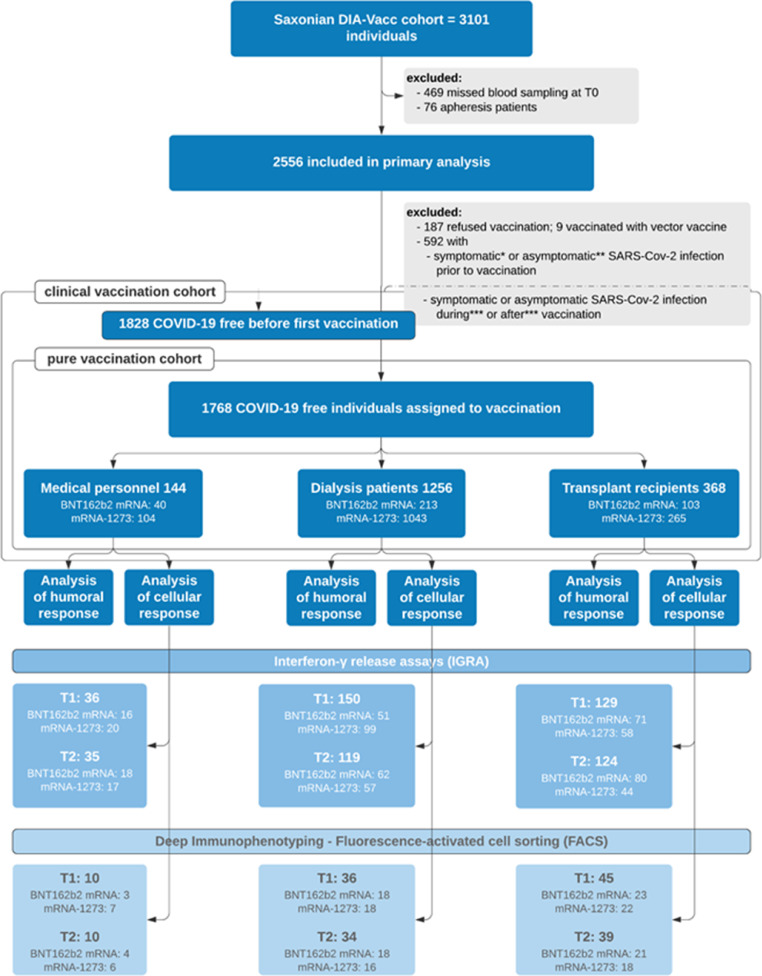
Methods: We conducted a prospective study exploring the eight week time course of specific cellular (interferon-γ release assay and flow cytometry) or/and humoral immune responses (ELISA) to SARS-CoV-2 boost vaccination in more than 3100 participants including medical personnel, dialysis patients and kidney transplant recipients using mRNA vaccines BNT162b2 or mRNA-1273.
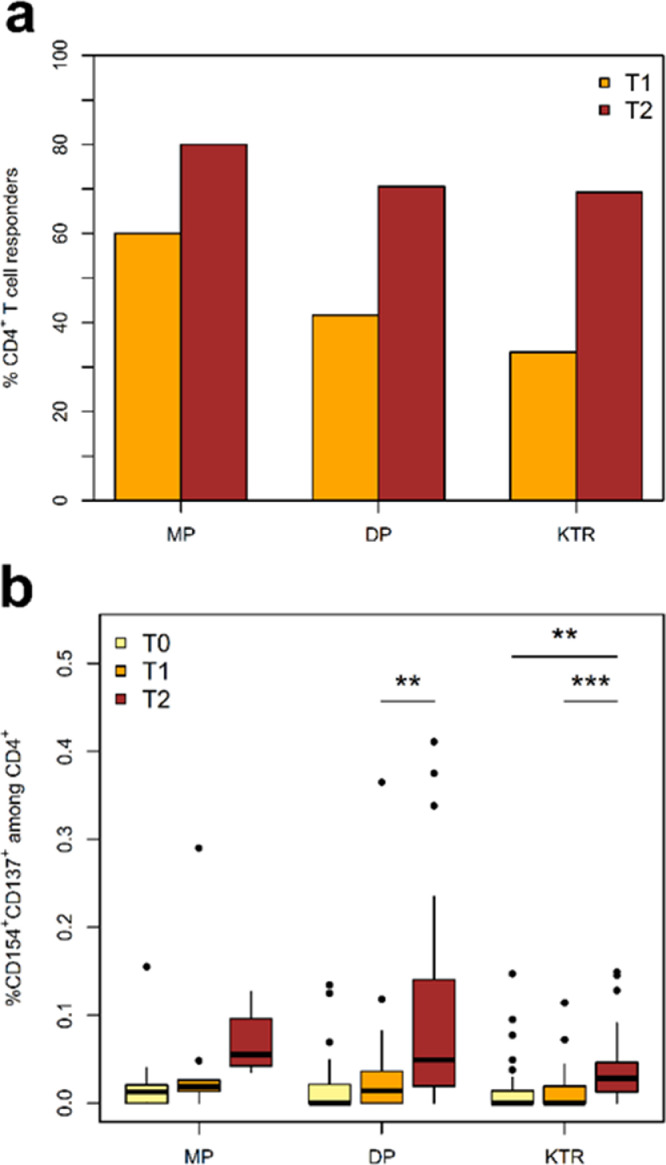
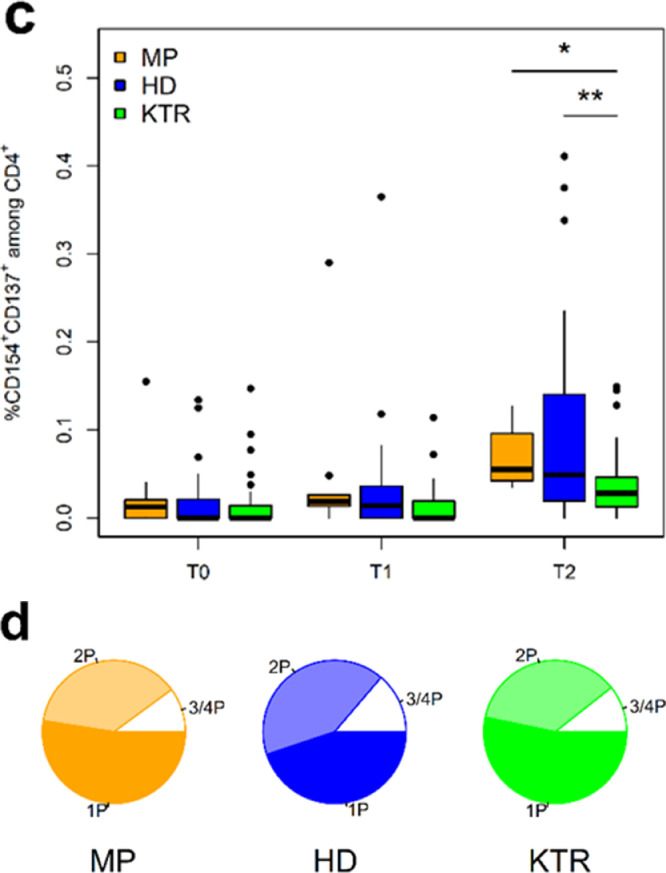
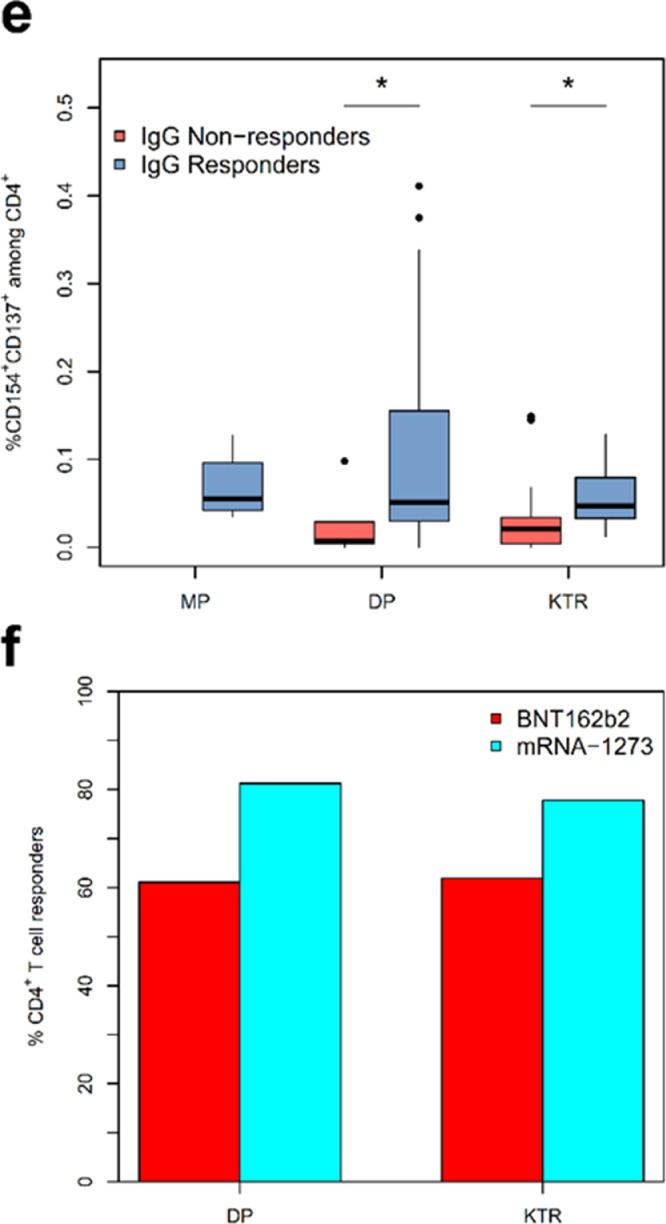
Results: SARS-CoV-2-vaccination induced seroconversion efficacy in dialysis patients was similar to medical personnel (> 95%), but markedly impaired in kidney transplant recipients (42%). T-cellular immunity largely mimicked humoral results. Major risk factors of seroconversion failure were immunosuppressive drug number and type (belatacept, MMF-MPA, calcineurin-inhibitors) as well as vaccine type (BNT162b2 mRNA). Seroconversion rates induced by mRNA-1273 compared to BNT162b2 vaccine were 97% to 88% (p < 0.001) in dialysis and 49% to 26% in transplant patients, respectively. Specific IgG directed against the new binding domain of the spike protein (RDB) were significantly higher in dialysis patients vaccinated by mRNA-1273 (95%) compared to BNT162b2 (85%, p < 0.001). Vaccination appeared safe and highly effective demonstrating an almost complete lack of symptomatic COVID-19 disease after boost vaccination as well as ceased disease incidences during third pandemic wave in dialysis patients.
Conclusion: Dialysis patients exhibit a remarkably high seroconversion rate of 95% after boost vaccination, while humoral response is impaired in the majority of transplant recipients. Immunosuppressive drug number and type as well as vaccine type (BNT162b2) are major determinants of seroconversion failure in both dialysis and transplant patients suggesting immune monitoring and adaption of vaccination protocols.
Keywords: BNT162b2; COVID-19; SARS-CoV-2 vaccination; clinical decision-making; dialysis patients; epidemiology; guidelines; humoral and cellular immune response; kidney transplant recipients; mRNA-1273; medical personnel; tozinameran.
© 2021 The Authors.
Conflict of interest statement
PA, NB, KB, IB, AB-N, SC, KE, RF-W, KF, FG, XG, CH, JH, CK, FK, AK, HK, TL, TL, HM, RM, FM, PM, AP, AP, FP, TP, HR, JS, HS, JS, HS, TS, JS, AS, TS, US, JS, TW, TT, LA, KA-R, MA have no conflict of interests. JB has a relationship with the German Ministry of Health via Hannover Medical School and receives study coordination and per-patient fees for Crit-CoV-U study (proteomic prediction of COVID-19 severity). The study has been supported by a grant from the Else-Kröner-Fresenius-Stiftung.
Figures
References
-
- Infektionsfälle in Sachsen - sachsen.de. 04.05.2021, 12:30 2021. https://www.coronavirus.sachsen.de/infektionsfaelle-in-sachsen-4151.html.
-
- Friedrich P., Sattler A., Muller K., Nienen M., Reinke P., Babel N. Comparing humoral and cellular immune response against HBV vaccine in kidney transplant patients. Am J Transpl. 2015;15(12):3157–3165. - PubMed
-
- Roch T., Giesecke-Thiel C., Blazquez-Navarro A. Generation of HBsAg-reactive T- and B-cells following HBV vaccination in serological non-responders under hemodialysis treatment. Eur J Immunol. 2021 - PubMed
-
- Hirzel C., Kumar D. Influenza vaccine strategies for solid organ transplant recipients. Curr Opin Infect Dis. 2018;31(4):309–315. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
