

Growth Hormone Receptor (Ghr) 6ω Pseudoexon Activation: A Novel Cause Of Severe Growth Hormone Insensitivity (Ghi)
- PMID: 34318893
- PMCID: PMC8684449
- DOI: 10.1210/clinem/dgab550
Growth Hormone Receptor (Ghr) 6ω Pseudoexon Activation: A Novel Cause Of Severe Growth Hormone Insensitivity (Ghi)
Abstract
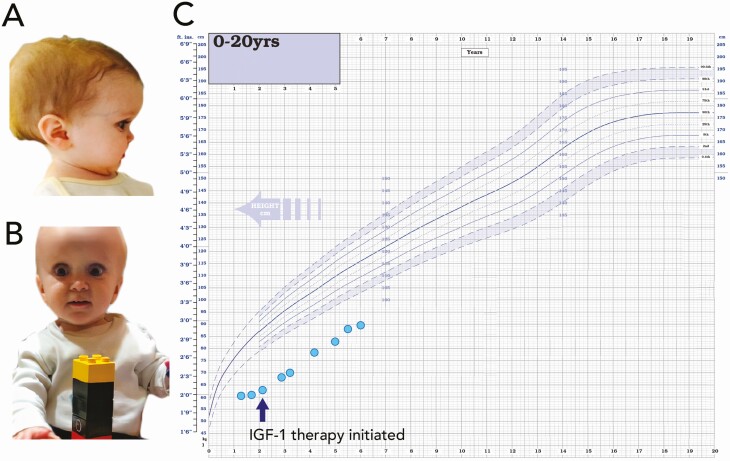
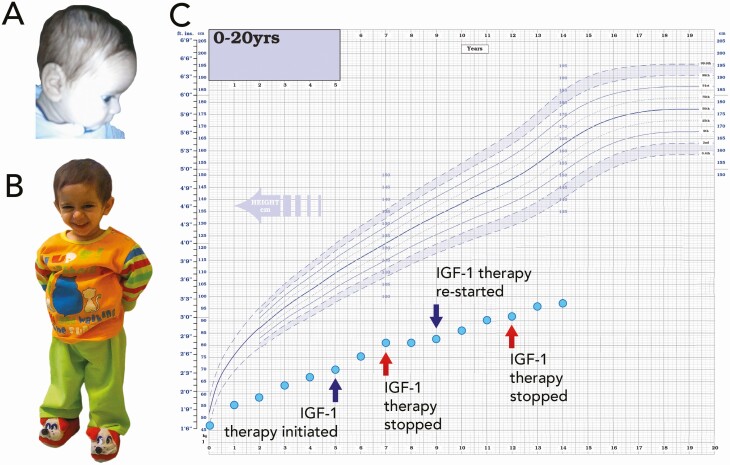
Context: Severe forms of Growth Hormone Insensitivity (GHI) are characterized by extreme short stature, dysmorphism and metabolic anomalies.
Objective: Identification of the genetic cause of growth failure in 3 'classical' GHI subjects.
Design: A novel intronic GHR variant was identified, and in vitro splicing assays confirmed aberrant splicing. A 6Ω pseudoexon GHR vector and patient fibroblast analysis assessed the consequences of the novel pseudoexon inclusion and the impact on GHR function.
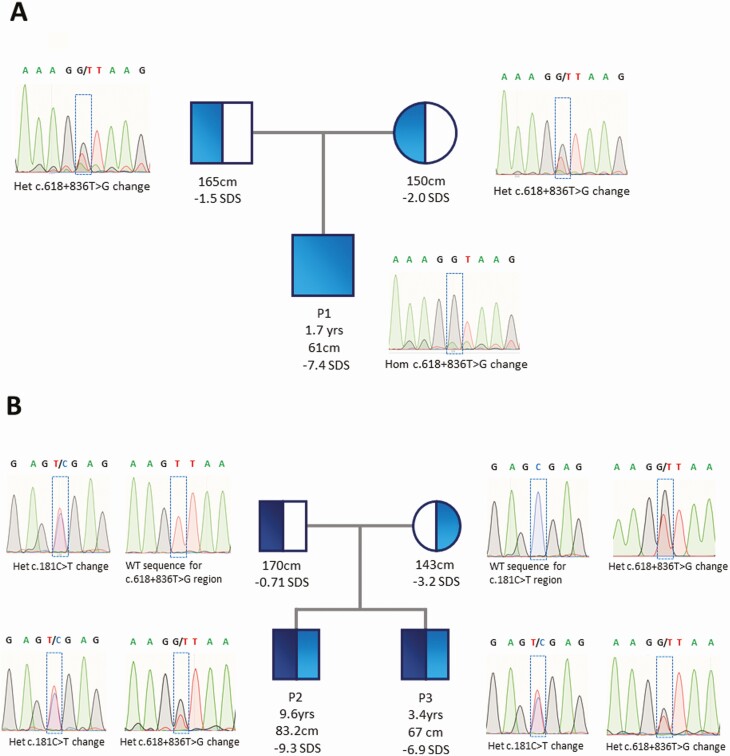
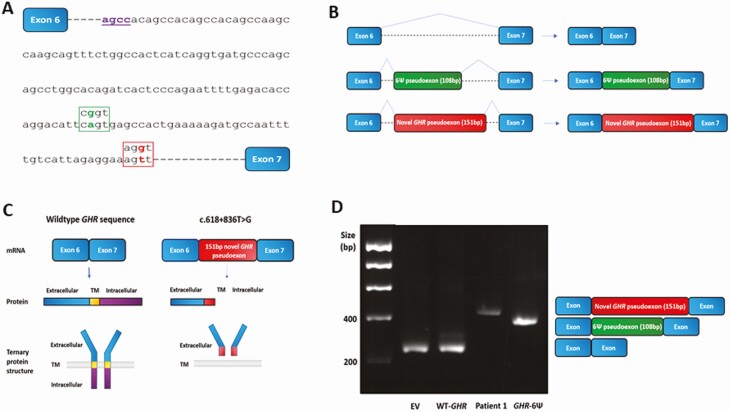
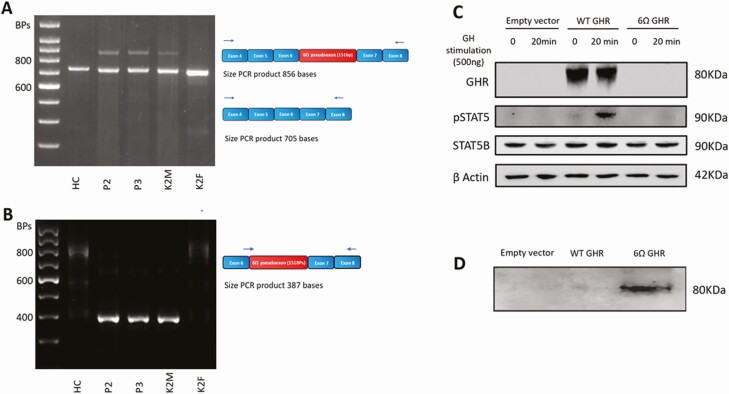
Results: We identified a novel homozygous intronic GHR variant (g.5:42700940T>G, c.618 + 836T> G), 44bp downstream of the previously recognized intronic 6Ψ GHR pseudoexon mutation in the index patient. Two siblings also harbored the novel intronic 6Ω pseudoexon GHR variant in compound heterozygosity with the known GHR c.181C>T (R43X) mutation. In vitro splicing analysis confirmed inclusion of a 151bp mutant 6Ω pseudoexon not identified in wild-type constructs. Inclusion of the 6Ω pseudoexon causes a frameshift resulting in a non-functional truncated GHR lacking the transmembrane and intracellular domains. The truncated 6Ω pseudoexon protein demonstrated extracellular accumulation and diminished activation of STAT5B signaling following growth hormone stimulation.
Conclusion: Novel GHR 6Ω pseudoexon inclusion results in loss of GHR function consistent with a severe GHI phenotype. This represents a novel mechanism of Laron syndrome and is the first deep intronic variant identified causing severe postnatal growth failure. The 2 kindreds originate from the same town in Campania, Southern Italy, implying common ancestry. Our findings highlight the importance of studying variation in deep intronic regions as a cause of monogenic disorders.
Keywords: GHR 6Ω pseudoexon; Short stature; growth hormone insensitivity; severe primary IGF-I deficiency.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Eshet R, Laron Z, Pertzelan A, Arnon R, Dintzman M. Defect of human growth hormone receptors in the liver of two patients with Laron-type dwarfism. Isr J Med Sci. 1984;20(1):8-11. - PubMed
-
- Laron Z, Pertzelan A, Mannheimer S. Genetic pituitary dwarfism with high serum concentation of growth hormone—a new inborn error of metabolism? Isr J Med Sci. 1966;2(2):152-155. - PubMed
-
- Berget SM. Exon recognition in vertebrate splicing. J Biol Chem. 1995;270(6):2411-2414. - PubMed
-
- Nakai K, Sakamoto H. Construction of a novel database containing aberrant splicing mutations of mammalian genes. Gene. 1994;141(2):171-177. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
