

Challenges of Estimating Accurate Prevalence of Arm Weakness Early After Stroke
- PMID: 34319189
- PMCID: PMC8442135
- DOI: 10.1177/15459683211028240
Challenges of Estimating Accurate Prevalence of Arm Weakness Early After Stroke
Abstract
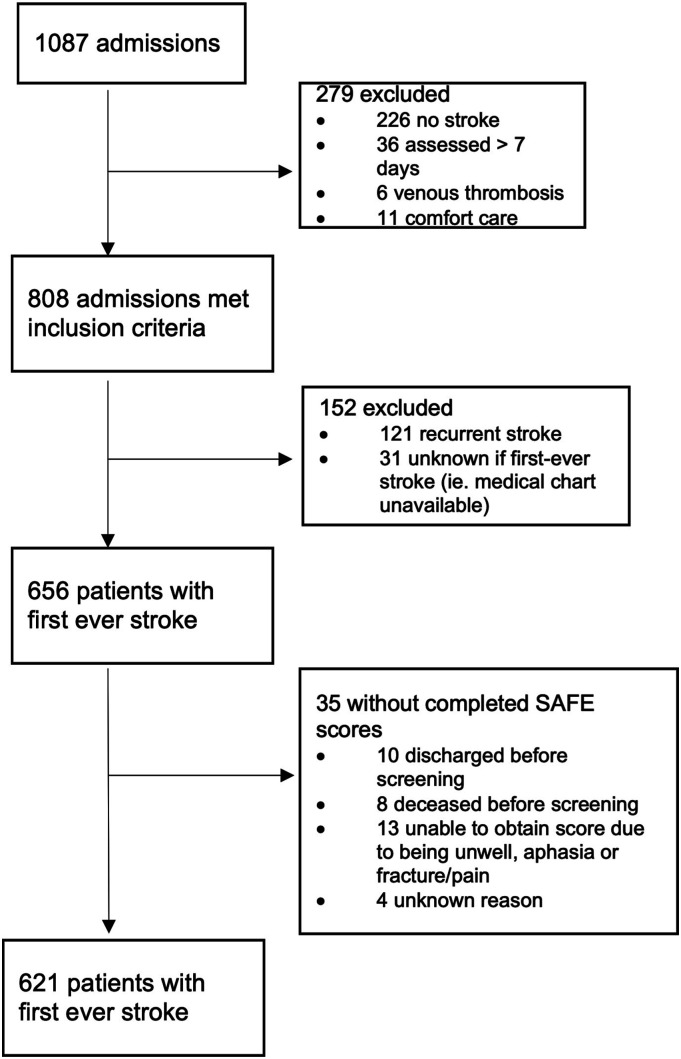
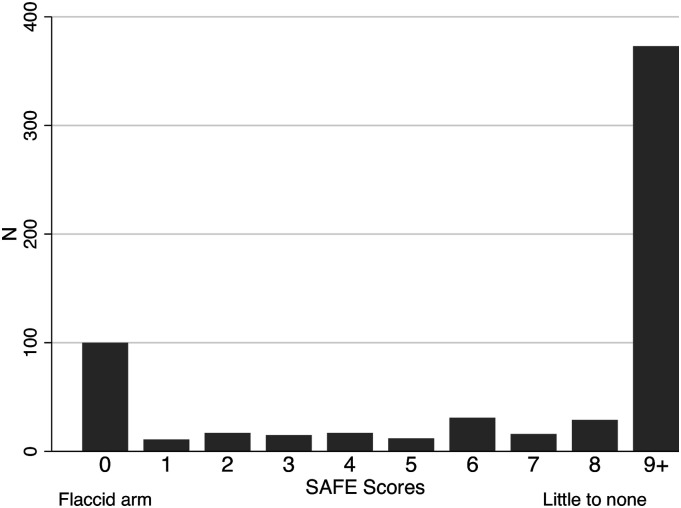
Background. Recent studies have reported lower statistics of upper limb (UL) weakness (48-57%) compared to widely cited values collected over 2 decades ago (70-80%). Objective. To explore potential factors contributing to the accuracy of prevalence values of UL weakness using a case study from a single regional centre. Methods. All patients admitted to the acute stroke unit with suspected diagnosis of stroke were screened from February 2016 to August 2017. Upper limb weakness was captured (a) prospectively using the Shoulder Abduction and Finger Extension (SAFE) score performed by unit physical therapists within 7 days post-stroke and (b) retrospectively via chart review using the National Institutes of Health Stroke Scale (NIHSS) arm score at admission and 24 hours post-admission. Results. A total of 656 patients were admitted with a first-ever stroke, and 621 (95%) individuals were administered the SAFE score. A total of 40% of individuals had UL weakness using the SAFE score (SAFE ≤8) at a mean time of 1.9 (SD 1.5) days post-stroke. In the same sample, 57% and 49% had UL weakness using the admission and 24-hour post-admission NIHSS arm score, respectively. Conclusions. The accuracy of population-level UL weakness prevalence values can be affected by weakness measure and score cut-off, time post-stroke weakness is captured, sample characteristics and use of single or multiple sites. Researchers using prevalence values for clinical trial planning should consider these attributes when using prevalence data for estimating recruitment rates and resource needs.
Keywords: prevalence; rehabilitation; stroke; upper extremity.
Conflict of interest statement
Figures
Similar articles
-
Prevalence of Arm Weakness, Pre-Stroke Outcomes and Other Post-Stroke Impairments Using Routinely Collected Clinical Data on an Acute Stroke Unit.Neurorehabil Neural Repair. 2024 Feb;38(2):148-160. doi: 10.1177/15459683241229676. Epub 2024 Feb 10. Neurorehabil Neural Repair. 2024. PMID: 38340009 Free PMC article.
-
Comparison of the action research arm test and the Fugl-Meyer assessment as measures of upper-extremity motor weakness after stroke.Arch Phys Med Rehabil. 2006 Jul;87(7):962-6. doi: 10.1016/j.apmr.2006.02.036. Arch Phys Med Rehabil. 2006. PMID: 16813784
-
A Self-Empowered Upper Limb Repetitive Engagement Program to Improve Upper Limb Recovery Early Post-Stroke: Phase II Pilot Randomized Controlled Trial.Neurorehabil Neural Repair. 2021 Sep;35(9):836-848. doi: 10.1177/15459683211032967. Epub 2021 Jul 19. Neurorehabil Neural Repair. 2021. PMID: 34281405 Clinical Trial.
-
Grip strength is a representative measure of muscle weakness in the upper extremity after stroke.Top Stroke Rehabil. 2016 Dec;23(6):400-405. doi: 10.1080/10749357.2016.1168591. Epub 2016 May 4. Top Stroke Rehabil. 2016. PMID: 27145212
-
Effects of Robot-Assisted Therapy for the Upper Limb After Stroke.Neurorehabil Neural Repair. 2017 Feb;31(2):107-121. doi: 10.1177/1545968316666957. Epub 2016 Sep 24. Neurorehabil Neural Repair. 2017. PMID: 27597165 Review.
Cited by
-
Considerations for developing complex post-stroke upper limb behavioural interventions: An international qualitative study.Clin Rehabil. 2024 Sep;38(9):1249-1263. doi: 10.1177/02692155241265271. Epub 2024 Jul 25. Clin Rehabil. 2024. PMID: 39053023 Free PMC article.
-
Distinguishing Distinct Neural Systems for Proximal vs Distal Upper Extremity Motor Control After Acute Stroke.Neurology. 2023 Jul 25;101(4):e347-e357. doi: 10.1212/WNL.0000000000207417. Epub 2023 Jun 2. Neurology. 2023. PMID: 37268437 Free PMC article.
-
The assistive potential of functional electrical stimulation to support object manipulation in functional upper extremity movements after stroke: A randomized cross-over study.J Cent Nerv Syst Dis. 2024 May 6;16:11795735241247812. doi: 10.1177/11795735241247812. eCollection 2024. J Cent Nerv Syst Dis. 2024. PMID: 38715966 Free PMC article.
-
Responsiveness and trajectory of changes in the rating of everyday arm-use in the community and home (REACH) scale over the first-year post-stroke.Clin Rehabil. 2023 Apr;37(4):557-568. doi: 10.1177/02692155221134413. Epub 2022 Oct 31. Clin Rehabil. 2023. PMID: 36310441 Free PMC article.
-
Virtual Arm Boot Camp (V-ABC): study protocol for a mixed-methods study to increase upper limb recovery after stroke with an intensive program coupled with a grasp count device.Trials. 2022 Feb 8;23(1):129. doi: 10.1186/s13063-022-06047-9. Trials. 2022. PMID: 35135585 Free PMC article.
References
-
- Nakayama H, Stig Jørgensen H, Otto Raaschou H, Skyhøj Olsen T. Recovery of upper extremity function in stroke patients: the Copenhagen Stroke study. Arch Phys Med Rehabil. 1994;75:394-398. - PubMed
-
- Kotila M, Waltimo O, Niemi ML, Laaksonen R, Lempinen M. The profile of recovery from stroke and factors influencing outcome. Stroke. 1984;15:1039-1044. - PubMed
-
- Lawrence ES, Coshall C, Dundas R, et al.. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke. 2001;32: 1279-1284. - PubMed
-
- Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of incident stroke signs and symptoms. Stroke 2002; 33: 2718-2721. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
