

Editorial
doi: 10.1016/j.xjtc.2020.12.043.
eCollection 2021 Jun.
Commissural geometry and cusp fusion insights to guide bicuspid aortic valve repair
Affiliations
- PMID: 34319302
- PMCID: PMC8311622
- DOI: 10.1016/j.xjtc.2020.12.043
Item in Clipboard
Editorial
Commissural geometry and cusp fusion insights to guide bicuspid aortic valve repair
JTCVS Tech.
.
No abstract available
Figures

Our new repair-oriented BAV classification. Range of commissural orientation 120° to 180°.

Our new repair-oriented BAV classification. Range of commissural orientation 120° to 180°. BAV, Bicuspid aortic valve.
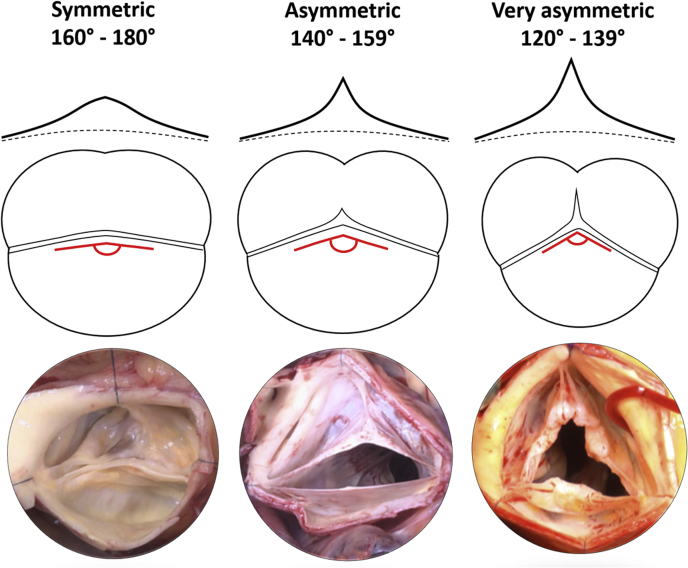
Repair-oriented classification of bicuspid aortic valve (BAV) phenotypes. Upper panel, Raphe height. Middle panel, Respective commissural orientation and raphe fusion. Lower panel, Surgical view of native valve.

Illustration of measurements of interest in bicuspid aortic valve (BAV) repair. Transesophageal echocardiographic assessment of commissural orientation (CO). Intraoperative measure of geometric height (gH) of fused cups (fc) and nonfused cusp (nfc) and length of cusp fusion line (LF); height of raphe (RH) and commissures (CH) in BAV.

Upper panel, transesophageal echocardiography assessment of commissural orientation on short axis in diastole; view from underneath the valve. Lower panel, Respective surgical view from above the valve.

Deep root dissection below the level of the ventriculo-aortic junction (VAJ) (dotted line), with separation of right- and left-ventricular outflow tracts. Placement of annuloplasty sutures at the level of the basal ring (interventricular septum [yellow arrows]).
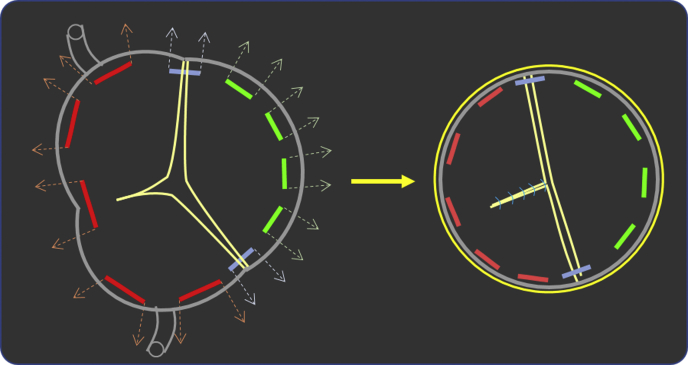
Placement of basal ring sutures in bicuspid aortic valve (BAV). Selective annuloplasty to achieve symmetry at the level of the basal ring, which also sets up correct 180° placement of the commissures (Valsalva graft [yellow ring]).

Symmetric phenotype; requires central plication with 180° reimplantation technique. A and B, One hundred seventy-degree bicuspid aortic valve (BAV) repaired with 180° reimplantation technique. C and D, One hundred sixty-degree BAV repaired with central plication of fused cusp and 180° reimplantation technique.

Asymmetric phenotype. (A-D) A, One hundred fifty-degree bicuspid aortic valve (BAV) with fusion right/left-cusp. B, Central plication with raphe thinning. C, Direct closure of unfused segment of fused cusp. D, One hundred eighty-degree reimplantation technique with plication of the nonfused cusp. (E-H) E, One hundred fifty-degree BAV with fusion of right/left cusps. F and G, Raphe thinning with direct closure. H, One hundred eighty-degree reimplantation technique. (I-L) I, One hundred forty-degree BAV with fusion of right/left-cusps. J, Central plication with raphe thinning. K, Direct closure of unfused segment of fused cusp. L, One hundred eighty-degree reimplantation technique with plication of the nonfused cusp.
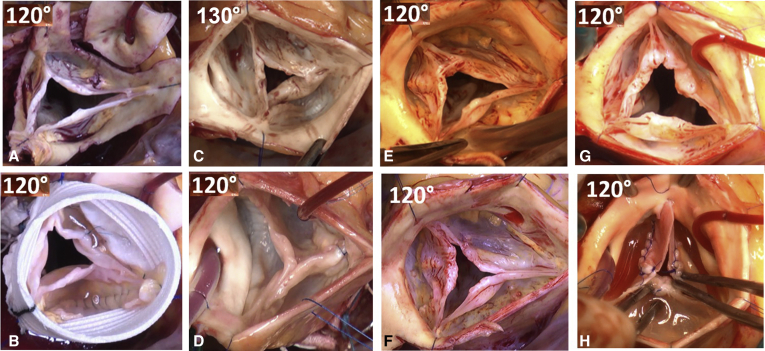
Very asymmetric phenotype requires a very tailored approach. In general, the 120° configuration is kept, and a new functional commissure is created by different techniques. A and B, Type fruste with commissurotomy, right coronary cusp central plication, and 120° reimplantation. C and D, Commissure resuspension. E and F, Commissurotomy and leaflet thinning. G and H, Commissure reconstruction with butterfly pericardial patch.

Very asymmetric fenestrated chord type. A through D, Cord resection, raphe direct closure. E through H, Cord resection, raphe direct closure, and 180° reimplantation technique.
Comment in
-
New horizons in aortic valve repair.JTCVS Tech. 2021 Apr 26;7:71. doi: 10.1016/j.xjtc.2021.04.018. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34471910 Free PMC article. No abstract available.
Comment on
-
Aortic annuloplasty: Subcommissural, intra-annular suture techniques, external and internal rings.JTCVS Tech. 2021 Jan 28;7:98-102. doi: 10.1016/j.xjtc.2020.12.044. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34318215 Free PMC article.
-
Cusp repair techniques in bicuspid and tricuspid aortic valves.JTCVS Tech. 2021 Jan 28;7:109-116. doi: 10.1016/j.xjtc.2021.01.029. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34318219 Free PMC article. No abstract available.
-
The art of aortic valve repair.JTCVS Tech. 2021 Jan 28;7:121-125. doi: 10.1016/j.xjtc.2021.01.030. eCollection 2021 Jun. JTCVS Tech. 2021. PMID: 34318222 Free PMC article. No abstract available.
References
-
- de Meester C., Pasquet A., Gerber B.L., Vancraeynest D., Noirhomme P., El Khoury G., et al. Valve repair improves the outcome of surgery for chronic severe aortic regurgitation: a propensity score analysis. J Thorac Cardiovasc Surg. 2014;148:1913–1920. - PubMed
-
- Arabkhani B., Mookhoek A., Di Centa I., Lansac E., Bekkers J.A., De Lind Van Wijngaarden R., et al. Reported outcome after valve-sparing aortic root replacement for aortic root aneurysm: a systematic review and meta-analysis. Ann Thorac Surg. 2015;100:1126–1131. - PubMed
-
- Aicher D., Holz A., Feldner S., Kollner V., Schafers H.J. Quality of life after aortic valve surgery: replacement versus reconstruction. J Thorac Cardiovasc Surg. 2011;142:e19–e24. - PubMed
-
- Mookhoek A., Korteland N.M., Arabkhani B., Di Centa I., Lansac E., Bekkers J.A., et al. Bentall procedure: a systematic review and meta-analysis. Ann Thorac Surg. 2016;101:1684–1689. - PubMed
-
- Wong C.H.M., Chan J.S.K., Sanli D., Rahimli R., Harky A. Aortic valve repair or replacement in patients with aortic regurgitation: a systematic review and meta-analysis. J Card Surg. 2019;34:377–384. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
