

Incidence of Infertility and Pregnancy Complications in US Female Surgeons
- PMID: 34319353
- PMCID: PMC9382914
- DOI: 10.1001/jamasurg.2021.3301
Incidence of Infertility and Pregnancy Complications in US Female Surgeons
Erratum in
-
Error in Results.JAMA Surg. 2021 Oct 1;156(10):991. doi: 10.1001/jamasurg.2021.4450. JAMA Surg. 2021. PMID: 34431988 Free PMC article. No abstract available.
Abstract
Importance: While surgeons often delay pregnancy and childbearing because of training and establishing early careers, little is known about risks of infertility and pregnancy complications among female surgeons.
Objective: To describe the incidence of infertility and pregnancy complications among female surgeons in the US and to identify workplace factors associated with increased risk compared with a sociodemographically similar nonsurgeon population.
Design, setting, and participants: This self-administered survey questionnaire was electronically distributed and collected from November 2020 to January 2021 through multiple surgical societies in the US and social media among male and female attending and resident surgeons with children. Nonchildbearing surgeons were asked to answer questions regarding the pregnancies of their nonsurgeon partners as applicable.
Exposures: Surgical profession; work, operative, and overnight call schedules.
Main outcomes and measures: Descriptive data on pregnancy loss were collected for female surgeons. Use of assisted reproductive technology was compared between male and female surgeons. Pregnancy and neonatal complications were compared between female surgeons and female nonsurgeon partners of surgeons.
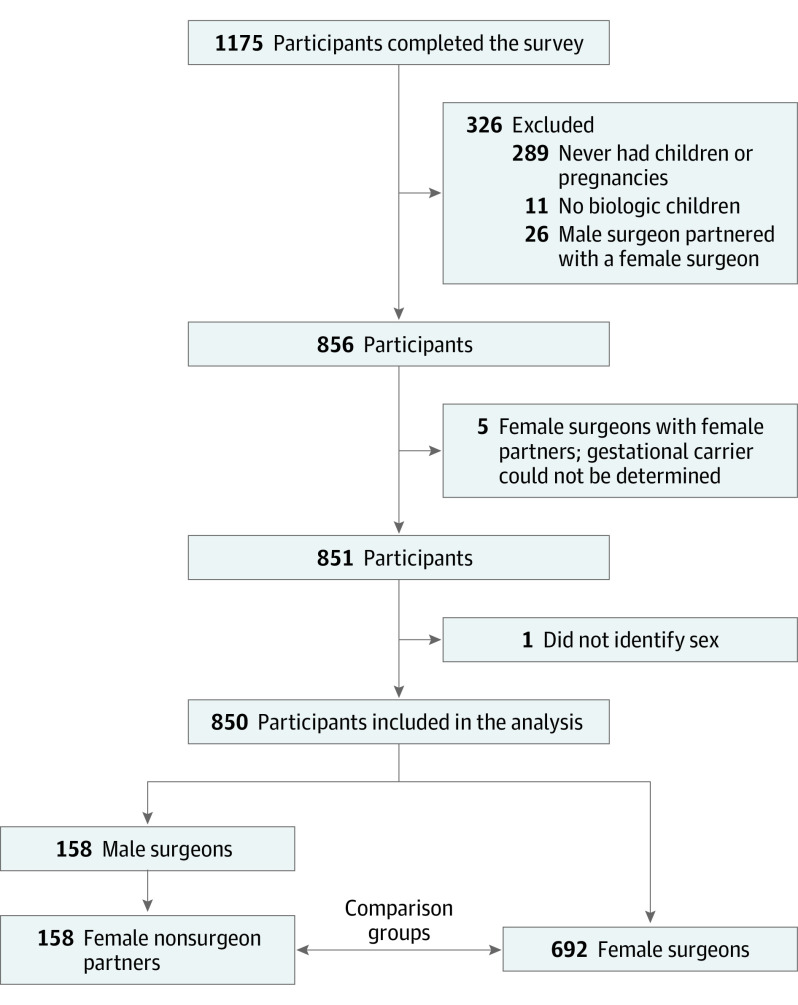
Results: A total of 850 surgeons (692 women and 158 men) were included in this survey study. Female surgeons with female partners were excluded because of lack of clarity about who carried the pregnancy. Because the included nonchildbearing population was therefore made up of male individuals with female partners, this group is referred to throughout the study as male surgeons. The median (IQR) age was 40 (36-45) years. Of 692 female surgeons surveyed, 290 (42.0%) had a pregnancy loss, more than twice the rate of the general population. Compared with male surgeons, female surgeons had fewer children (mean [SD], 1.8 [0.8] vs 2.3 [1.1]; P < .001), were more likely to delay having children because of surgical training (450 of 692 [65.0%] vs 69 of 158 [43.7%]; P < .001), and were more likely to use assisted reproductive technology (172 of 692 [24.9%] vs 27 of 158 [17.1%]; P = .04). Compared with female nonsurgeon partners, female surgeons were more likely to have major pregnancy complications (311 of 692 [48.3%] vs 43 of 158 [27.2%]; P < .001), which was significant after controlling for age, work hours, in vitro fertilization use, and multiple gestation (odds ratio [OR], 1.72; 95% CI, 1.11-2.66). Female surgeons operating 12 or more hours per week during the last trimester of pregnancy were at higher risk of major pregnancy complications compared with those operating less than 12 hours per week (OR, 1.57; 95% CI, 1.08-2.26). Compared with female nonsurgeon partners, female surgeons were more likely to have musculoskeletal disorders (255 of 692 [36.9%] vs 29 of 158 [18.4%]; P < .001), nonelective cesarean delivery (170 of 692 [25.5%] vs 24 of 158 [15.3%]; P = .01), and postpartum depression (77 of 692 [11.1%] vs 9 of 158 [5.7%]; P = .04).
Conclusions and relevance: This national survey study highlighted increased medical risks of infertility and pregnancy complications among female surgeons. With an increasing percentage of women representing the surgical workforce, changing surgical culture to support pregnancy is paramount to reducing the risk of major pregnancy complications, use of fertility interventions, or involuntary childlessness because of delayed attempts at childbearing.
Conflict of interest statement
Figures
Comment in
-
When Leaning In Becomes Unhealthy, Can We Fix It?JAMA Surg. 2021 Oct 1;156(10):915-916. doi: 10.1001/jamasurg.2021.3302. JAMA Surg. 2021. PMID: 34319401 No abstract available.
-
Comments on Study About US Female Surgeons.JAMA Surg. 2022 Apr 1;157(4):358. doi: 10.1001/jamasurg.2021.6447. JAMA Surg. 2022. PMID: 34964816 No abstract available.
-
Comments on Study About US Female Surgeons.JAMA Surg. 2022 Apr 1;157(4):357-358. doi: 10.1001/jamasurg.2021.6446. JAMA Surg. 2022. PMID: 34964817 No abstract available.
-
Comments on Study About US Female Surgeons-Reply.JAMA Surg. 2022 Apr 1;157(4):358-359. doi: 10.1001/jamasurg.2021.6448. JAMA Surg. 2022. PMID: 34964830 No abstract available.
References
-
- Association of American Medical Colleges . US medical school applicants, matriculants, and graduates by gender, academic year, 2018-2019. Accessed February 27, 2021. https://www.aamc.org/media/43351/download
-
- Association of American Medical Colleges . The state of women in academic medicine 2018-2019: percentage of women residents by specialty, 2018. Accessed February 27,2021. https://www.aamc.org/data-reports/data/2018-2019-state-women-academic-me...
-
- American College of Surgeons. 2018 ACS governors survey: gender inequality and harassment remain a challenge in surgery. Accessed March 1, 2021. https://bulletin.facs.org/2019/09/2018-acs-governors-survey-gender-inequ...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
