

Using Consistently Low Performance to Identify Low-Quality Physician Groups
- PMID: 34319356
- PMCID: PMC8319756
- DOI: 10.1001/jamanetworkopen.2021.17954
Using Consistently Low Performance to Identify Low-Quality Physician Groups
Abstract
Importance: There has been a growth in the use of performance-based payment models in the past decade, but inherently noisy and stochastic quality measures complicate the assessment of the quality of physician groups. Examining consistently low performance across multiple measures or multiple years could potentially identify a subset of low-quality physician groups.
Objective: To identify low-performing physician groups based on consistently low performance after adjusting for patient characteristics across multiple measures or multiple years for 10 commonly used quality measures for diabetes and cardiovascular disease (CVD).
Design, setting, and participants: This cross-sectional study used medical and pharmacy claims and laboratory data for enrollees ages 18 to 65 years with diabetes or CVD in an Aetna health insurance plan between 2016 and 2019. Each physician group's risk-adjusted performance for a given year was estimated using mixed-effects linear probability regression models. Performance was correlated across measures and time, and the proportion of physician groups that performed in the bottom quartile was examined across multiple measures or multiple years. Data analysis was conducted between September 2020 and May 2021.
Exposures: Primary care physician groups.
Main outcomes and measures: Performance scores of 6 quality measures for diabetes and 4 for CVD, including hemoglobin A1c (HbA1c) testing, low-density lipoprotein testing, statin use, HbA1c control, low-density lipoprotein control, and hospital-based utilization.
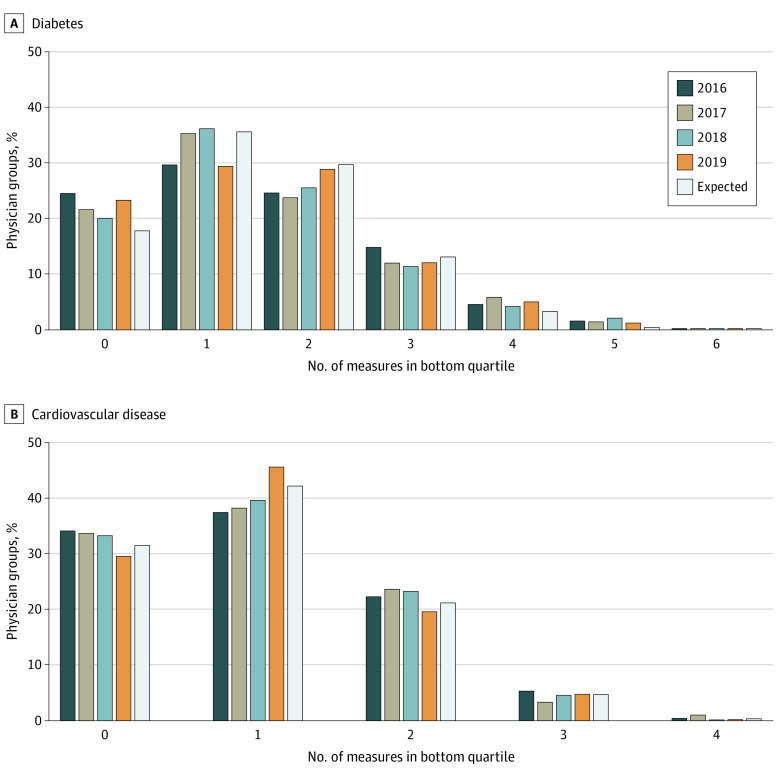
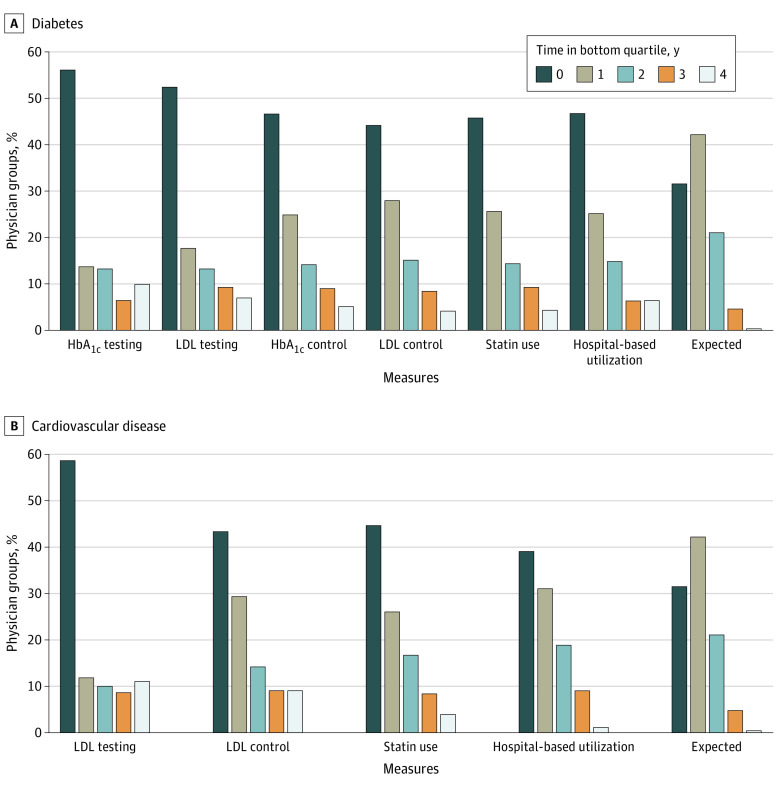
Results: A total of 786 641 unique enrollees treated by 890 physician groups were included; 414 655 (52.7%) of the enrollees were men and the mean (SD) age was 53 (9.5) years. After adjusting for age, sex, and clinical and social risk variables, correlations among individual measures were weak (eg, performance-adjusted correlation between any statin use and LDL testing for patients with diabetes, r = -0.10) to moderate (correlation between LDL testing for diabetes and LDL testing for CVD, r = .43), but year-to-year correlations for all measures were moderate to strong. One percent or fewer of physician groups performed in the bottom quartile for all 6 diabetes measures or all 4 cardiovascular disease measures in any given year, while 14 (4.0%) to 39 groups (11.1%) were in the bottom quartile in all 4 years for any given measure other than hospital-based utilization for CVD (1.1%).
Conclusions and relevance: A subset of physician groups that was consistently low performing could be identified by considering performance measures across multiple years. Considering the consistency of group performance could contribute a novel method to identify physician groups most likely to benefit from limited resources.
Conflict of interest statement
Figures
Similar articles
-
Social Risk Adjustment of Quality Measures for Diabetes and Cardiovascular Disease in a Commercially Insured US Population.JAMA Netw Open. 2019 Mar 1;2(3):e190838. doi: 10.1001/jamanetworkopen.2019.0838. JAMA Netw Open. 2019. PMID: 30924891 Free PMC article.
-
Association Between Clinical Practice Group Adherence to Quality Measures and Adverse Outcomes Among Adult Patients With Diabetes.JAMA Netw Open. 2019 Aug 2;2(8):e199139. doi: 10.1001/jamanetworkopen.2019.9139. JAMA Netw Open. 2019. PMID: 31411713 Free PMC article.
-
The unreliability of individual physician "report cards" for assessing the costs and quality of care of a chronic disease.JAMA. 1999 Jun 9;281(22):2098-105. doi: 10.1001/jama.281.22.2098. JAMA. 1999. PMID: 10367820
-
Payment methods for healthcare providers working in outpatient healthcare settings.Cochrane Database Syst Rev. 2021 Jan 20;1(1):CD011865. doi: 10.1002/14651858.CD011865.pub2. Cochrane Database Syst Rev. 2021. PMID: 33469932 Free PMC article.
-
Effects of pay-for-performance for primary care physicians on diabetes outcomes in single-payer health systems: a systematic review.Eur J Health Econ. 2019 Dec;20(9):1303-1315. doi: 10.1007/s10198-019-01097-4. Epub 2019 Aug 10. Eur J Health Econ. 2019. PMID: 31401699
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
