

Association Between Mood Disorders and Risk of COVID-19 Infection, Hospitalization, and Death: A Systematic Review and Meta-analysis
- PMID: 34319365
- PMCID: PMC8319830
- DOI: 10.1001/jamapsychiatry.2021.1818
Association Between Mood Disorders and Risk of COVID-19 Infection, Hospitalization, and Death: A Systematic Review and Meta-analysis
Abstract
Importance: Preexisting noncommunicable diseases (eg, diabetes) increase the risk of COVID-19 infection, hospitalization, and death. Mood disorders are associated with impaired immune function and social determinants that increase the risk of COVID-19. Determining whether preexisting mood disorders represent a risk of COVID-19 would inform public health priorities.
Objective: To assess whether preexisting mood disorders are associated with a higher risk of COVID-19 susceptibility, hospitalization, severe complications, and death.
Data sources: Systematic searches were conducted for studies reporting data on COVID-19 outcomes in populations with and without mood disorders on PubMed/MEDLINE, The Cochrane Library, PsycInfo, Embase, Web of Science, Google/Google Scholar, LitCovid, and select reference lists. The search timeline was from database inception to February 1, 2021.
Study selection: Primary research articles that reported quantitative COVID-19 outcome data in persons with mood disorders vs persons without mood disorders of any age, sex, and nationality were selected. Of 1950 articles identified through this search strategy, 21 studies were included in the analysis.
Data extraction and synthesis: The modified Newcastle-Ottawa Scale was used to assess methodological quality and risk of bias of component studies. Reported adjusted odds ratios (ORs) were pooled with unadjusted ORs calculated from summary data to generate 4 random-effects summary ORs, each corresponding to a primary outcome.
Main outcomes and measures: The 4 a priori primary outcomes were COVID-19 susceptibility, COVID-19 hospitalization, COVID-19 severe events, and COVID-19 death. The hypothesis was formulated before study search. Outcome measures between individuals with and without mood disorders were compared.
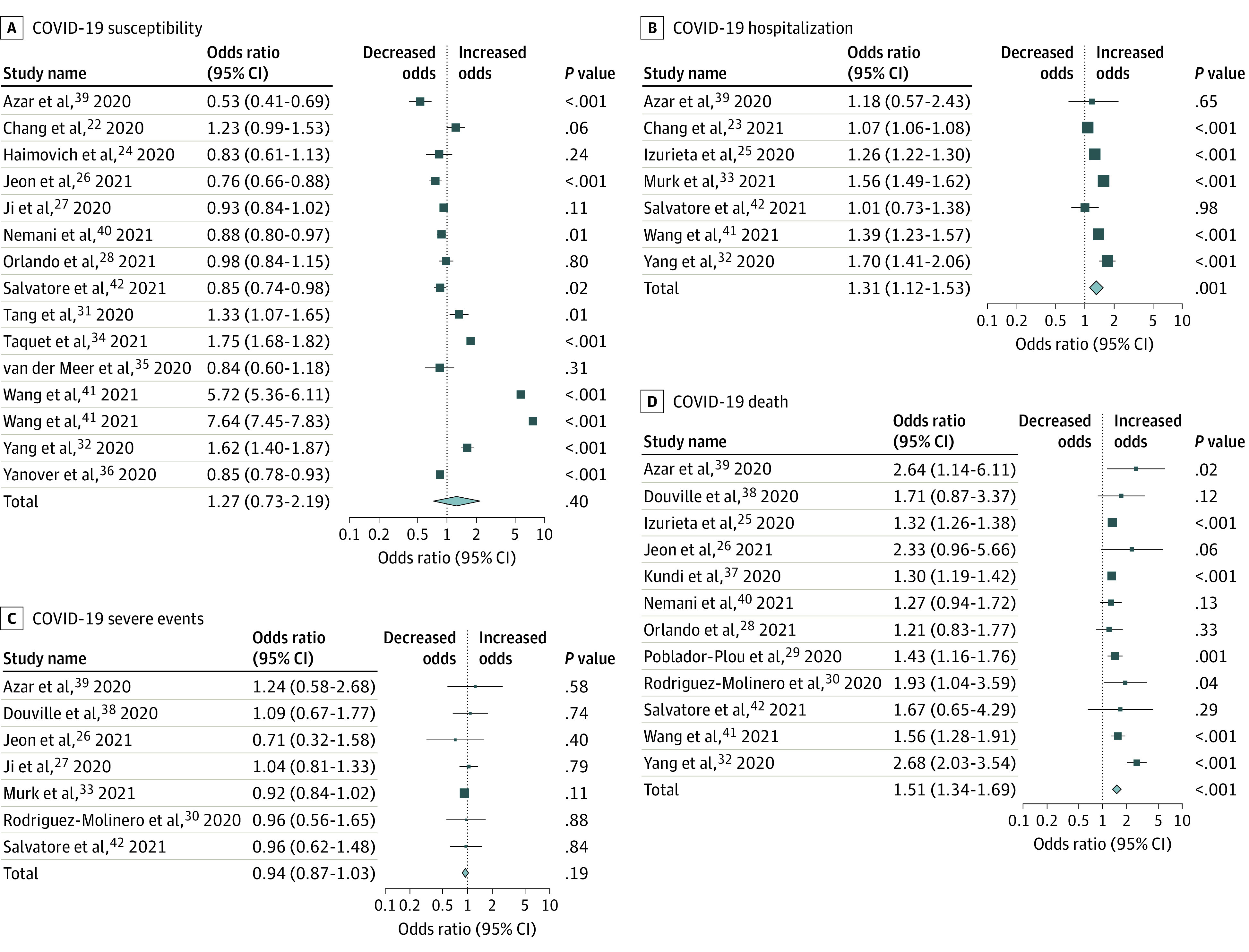
Results: This review included 21 studies that involved more than 91 million individuals. Significantly higher odds of COVID-19 hospitalization (OR, 1.31; 95% CI, 1.12-1.53; P = .001; n = 26 554 397) and death (OR, 1.51; 95% CI, 1.34-1.69; P < .001; n = 25 808 660) were found in persons with preexisting mood disorders compared with those without mood disorders. There was no association between mood disorders and COVID-19 susceptibility (OR, 1.27; 95% CI, 0.73-2.19; n = 65 514 469) or severe events (OR, 0.94; 95% CI, 0.87-1.03; n = 83 240). Visual inspection of the composite funnel plot for asymmetry indicated the presence of publication bias; however, the Egger regression intercept test result was not statistically significant.
Conclusions and relevance: The results of this systematic review and meta-analysis examining the association between preexisting mood disorders and COVID-19 outcomes suggest that individuals with preexisting mood disorders are at higher risk of COVID-19 hospitalization and death and should be categorized as an at-risk group on the basis of a preexisting condition.
Conflict of interest statement
Figures

References
-
- Keaten J. WHO: 10% of world’s people may have been infected with virus. Associated Press website. Updated 2020. Accessed February 15, 2020. https://apnews.com/article/virus-outbreak-archive-united-nations-54a3a58...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
