

Immersive virtual reality enables technical skill acquisition for scrub nurses in complex revision total knee arthroplasty
- PMID: 34319473
- PMCID: PMC8317146
- DOI: 10.1007/s00402-021-04050-4
Immersive virtual reality enables technical skill acquisition for scrub nurses in complex revision total knee arthroplasty
Abstract
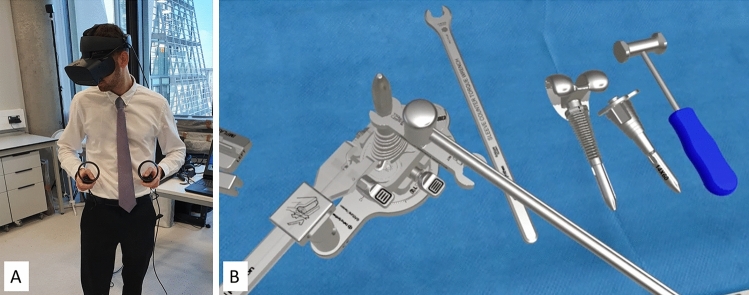
Introduction: Immersive Virtual Reality (iVR) is a novel technology which can enhance surgical training in a virtual environment without supervision. However, it is untested for the training to select, assemble and deliver instrumentation in orthopaedic surgery-typically performed by scrub nurses. This study investigates the impact of an iVR curriculum on this facet of the technically demanding revision total knee arthroplasty.
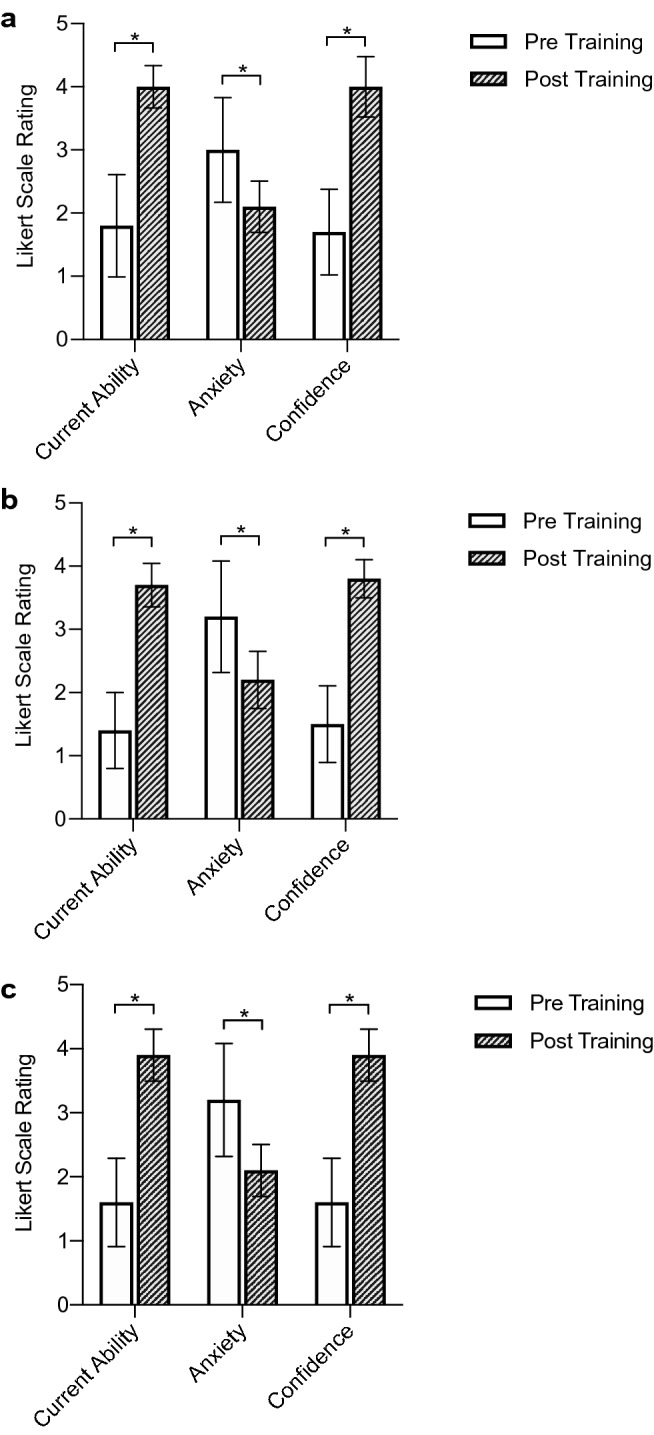
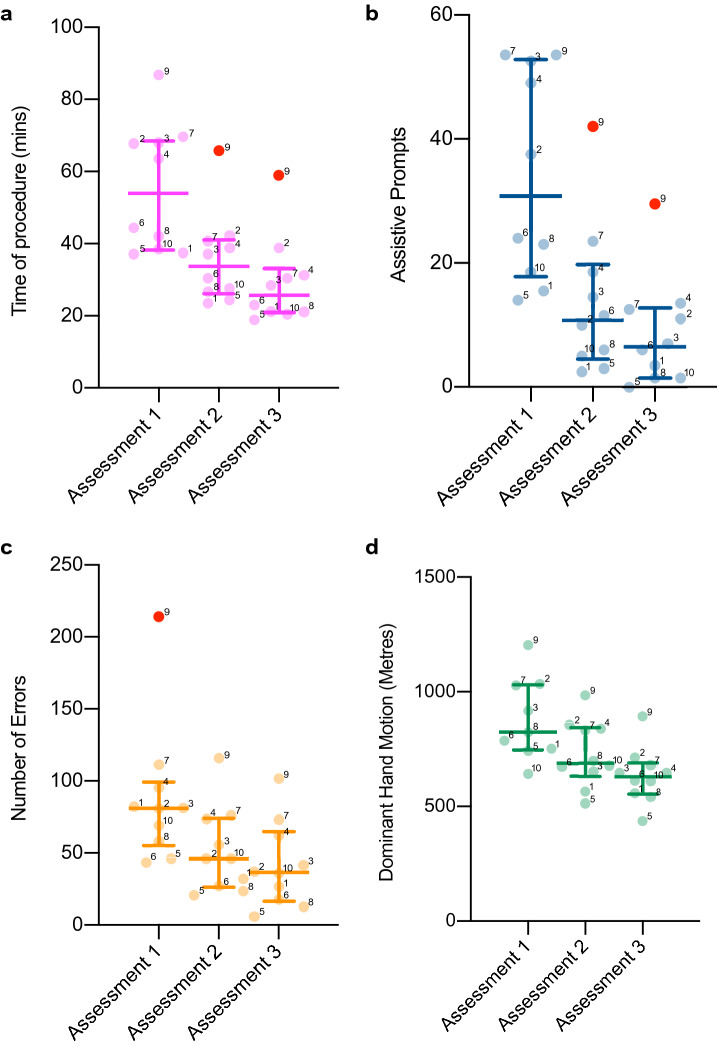
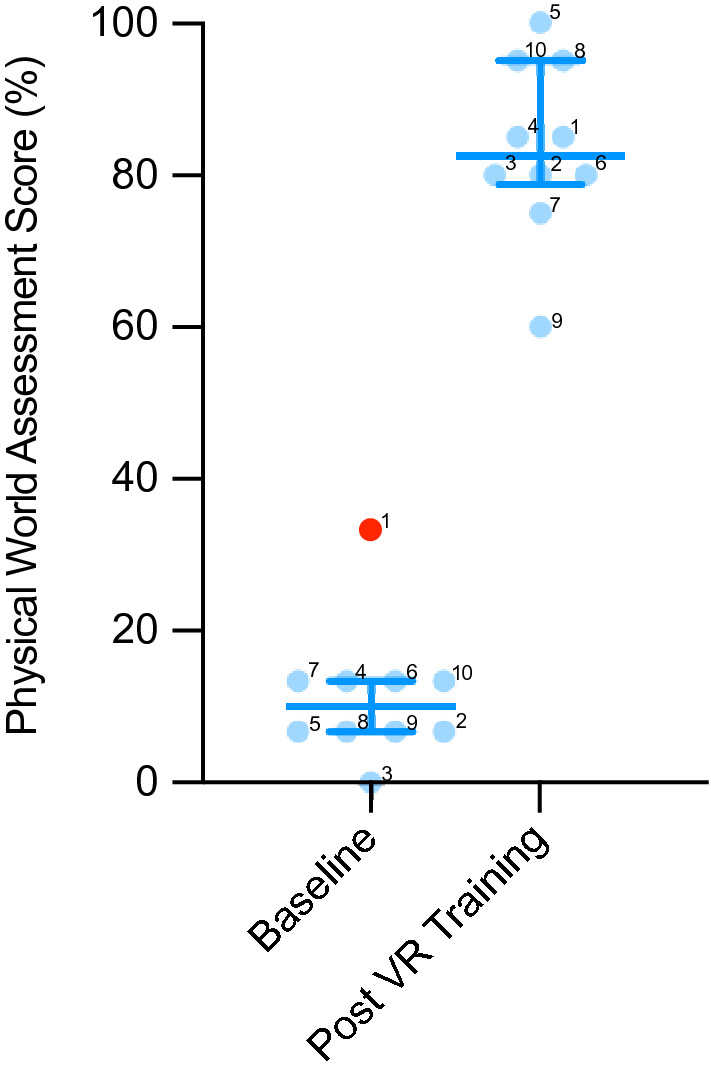
Materials and methods: Ten scrub nurses completed training in four iVR sessions over a 4-week period. Initially, nurses completed a baseline real-world assessment, performing their role with real equipment in a simulated operation assessment. Each subsequent iVR session involved a guided mode, where the software taught participants the procedural choreography and assembly of instrumentation in a simulated operating room. In the latter three sessions, nurses also undertook an assessment in iVR. Outcome measures were related to procedural sequence, duration of surgery and efficiency of movement. Transfer of skills from iVR to the real world was assessed in a post-training simulated operation assessment. A pre- and post-training questionnaire assessed the participants knowledge, confidence and anxiety.
Results: Operative time reduced by an average of 47% across the 3 unguided sessions (mean 55.5 ± 17.6 min to 29.3 ± 12.1 min, p > 0.001). Assistive prompts reduced by 75% (34.1 ± 16.8 to 8.6 ± 8.8, p < 0.001), dominant hand motion by 28% (881.3 ± 178.5 m to 643.3 ± 119.8 m, p < 0.001) and head motion by 36% (459.9 ± 99.7 m to 292.6 ± 85.3 m, p < 0.001). Real-world skill improved from 11% prior to iVR training to 84% correct post-training. Participants reported increased confidence and reduced anxiety in scrubbing for rTKA procedures (p < 0.001).
Conclusions: For scrub nurses, unfamiliarity with complex surgical procedures or equipment is common. Immersive VR training improved their understanding, technical skills and efficiency. These iVR-learnt skills transferred into the real world.
Keywords: Patient safety; Revision total knee arthroplasty; Simulation; Virtual reality.
© 2021. The Author(s).
Conflict of interest statement
T.C.E declares research funding from Johnson & Johnson, A.D.L declares research funding from the Royal College of Surgeons of England, J.P.C declares research funding and paid consultancy from Johnson & Johnson, Zimmer Biomet and JRI, he declares shares/stock in Embody Orthopaedic. K.L declares research funding from Johnson & Johnson, and the Royal College of Surgeons Royal College of Surgeons of England.
Figures
Similar articles
-
Fully Immersive Virtual Reality for Total Hip Arthroplasty: Objective Measurement of Skills and Transfer of Visuospatial Performance After a Competency-Based Simulation Curriculum.J Bone Joint Surg Am. 2020 Mar 18;102(6):e27. doi: 10.2106/JBJS.19.00629. J Bone Joint Surg Am. 2020. PMID: 31929324
-
Effectiveness of Immersive Virtual Reality on Orthopedic Surgical Skills and Knowledge Acquisition Among Senior Surgical Residents: A Randomized Clinical Trial.JAMA Netw Open. 2020 Dec 1;3(12):e2031217. doi: 10.1001/jamanetworkopen.2020.31217. JAMA Netw Open. 2020. PMID: 33369660 Free PMC article. Clinical Trial.
-
Collaborative Team Training in Virtual Reality is Superior to Individual Learning For Performing Complex Open Surgery: A Randomized Controlled Trial.Ann Surg. 2023 Dec 1;278(6):850-857. doi: 10.1097/SLA.0000000000006079. Epub 2023 Aug 28. Ann Surg. 2023. PMID: 37638414 Free PMC article. Clinical Trial.
-
Virtual and augmented reality for surgical training and simulation in knee arthroplasty.Arch Orthop Trauma Surg. 2021 Dec;141(12):2303-2312. doi: 10.1007/s00402-021-04037-1. Epub 2021 Jul 15. Arch Orthop Trauma Surg. 2021. PMID: 34264380 Review.
-
A Systematic Review of Immersive Virtual Reality for Nontechnical Skills Training in Surgery.J Surg Educ. 2024 Jan;81(1):25-36. doi: 10.1016/j.jsurg.2023.11.012. Epub 2023 Nov 30. J Surg Educ. 2024. PMID: 38036388
Cited by
-
Causes and associations with mortality in patients with pelvic ring injuries with haemorrhagic shock.Eur J Orthop Surg Traumatol. 2023 Oct;33(7):2971-2979. doi: 10.1007/s00590-023-03516-y. Epub 2023 Mar 16. Eur J Orthop Surg Traumatol. 2023. PMID: 36922411
-
Leading Transformation in Medical Education Through Extended Reality.Adv Exp Med Biol. 2023;1421:161-173. doi: 10.1007/978-3-031-30379-1_7. Adv Exp Med Biol. 2023. PMID: 37524987
-
Integration of Square Fiducial Markers in Patient-Specific Instrumentation and Their Applicability in Knee Surgery.J Pers Med. 2023 Apr 25;13(5):727. doi: 10.3390/jpm13050727. J Pers Med. 2023. PMID: 37240897 Free PMC article.
-
Role of eXtended Reality use in medical imaging interpretation for pre-surgical planning and intraoperative augmentation.J Med Imaging (Bellingham). 2024 Nov;11(6):062607. doi: 10.1117/1.JMI.11.6.062607. Epub 2024 Dec 5. J Med Imaging (Bellingham). 2024. PMID: 39649776 Review.
-
Virtual and augmented reality for anxiety reduction in orthopedic patients and providers: a systematic review.J Orthop Surg Res. 2025 Mar 31;20(1):327. doi: 10.1186/s13018-025-05690-7. J Orthop Surg Res. 2025. PMID: 40165273 Free PMC article.
References
-
- Sari AB, Sheldon TA, Cracknell A, Turnbull A. Sensitivity of routine system for reporting patient safety incidents in an NHS hospital: retrospective patient case note review. BMJ. 2007;334(7584):79. doi: 10.1136/bmj.39031.507153.AE. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
