

Impact of assessment and intervention by a health and social care professional team in the emergency department on the quality, safety, and clinical effectiveness of care for older adults: A randomised controlled trial
- PMID: 34319971
- PMCID: PMC8318294
- DOI: 10.1371/journal.pmed.1003711
Impact of assessment and intervention by a health and social care professional team in the emergency department on the quality, safety, and clinical effectiveness of care for older adults: A randomised controlled trial
Abstract
Background: Older adults frequently attend the emergency department (ED) and experience high rates of adverse events following ED presentation. This randomised controlled trial evaluated the impact of early assessment and intervention by a dedicated team of health and social care professionals (HSCPs) in the ED on the quality, safety, and clinical effectiveness of care of older adults in the ED.
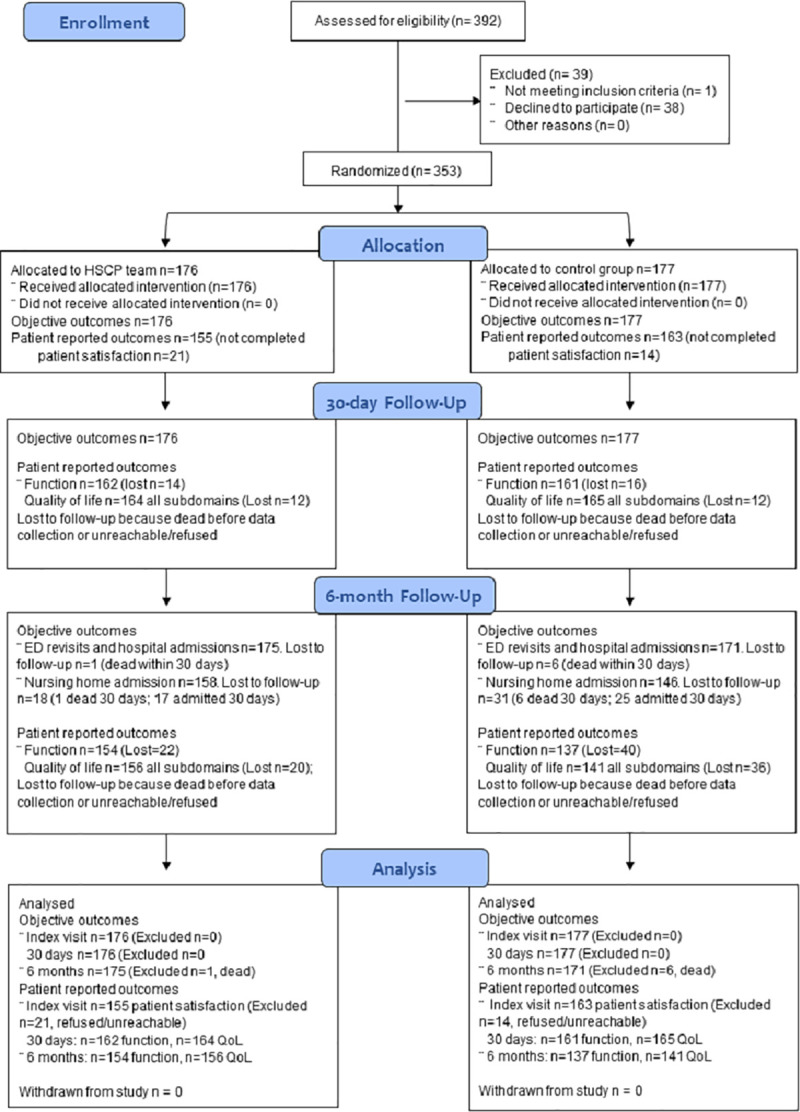
Methods and findings: This single-site randomised controlled trial included a sample of 353 patients aged ≥65 years (mean age = 79.6, SD = 7.01; 59.2% female) who presented with lower urgency complaints to the ED a university hospital in the Mid-West region of Ireland, during HSCP operational hours. The intervention consisted of early assessment and intervention carried out by a HSCP team comprising a senior medical social worker, senior occupational therapist, and senior physiotherapist. The primary outcome was ED length of stay. Secondary outcomes included rates of hospital admissions from the ED; hospital length of stay for admitted patients; patient satisfaction with index visit; ED revisits, mortality, nursing home admission, and unscheduled hospital admission at 30-day and 6-month follow-up; and patient functional status and quality of life (at index visit and follow-up). Demographic information included the patient's gender, age, marital status, residential status, mode of arrival to the ED, source of referral, index complaint, triage category, falls, and hospitalisation history. Participants in the intervention group (n = 176) experienced a significantly shorter ED stay than the control group (n = 177) (6.4 versus 12.1 median hours, p < 0.001). Other significant differences (intervention versus control) included lower rates of hospital admissions from the ED (19.3% versus 55.9%, p < 0.001), higher levels of satisfaction with the ED visit (p = 0.008), better function at 30-day (p = 0.01) and 6-month follow-up (p = 0.03), better mobility (p = 0.02 at 30 days), and better self-care (p = 0.03 at 30 days; p = 0.009 at 6 months). No differences at follow-up were observed in terms of ED re-presentation or hospital admission. Study limitations include the inability to blind patients or ED staff to allocation due to the nature of the intervention, and a focus on early assessment and intervention in the ED rather than care integration following discharge.
Conclusions: Early assessment and intervention by a dedicated ED-based HSCP team reduced ED length of stay and the risk of hospital admissions among older adults, as well as improving patient satisfaction. Our findings support the effectiveness of an interdisciplinary model of care for key ED outcomes.
Trial registration: ClinicalTrials.gov NCT03739515; registered on 12 November 2018.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
