

High mortality among kidney transplant recipients diagnosed with coronavirus disease 2019: Results from the Brazilian multicenter cohort study
- PMID: 34320005
- PMCID: PMC8318290
- DOI: 10.1371/journal.pone.0254822
High mortality among kidney transplant recipients diagnosed with coronavirus disease 2019: Results from the Brazilian multicenter cohort study
Abstract
Background: Kidney transplant (KT) recipients are considered a high-risk group for unfavorable outcomes in the course of coronavirus disease 2019 (COVID-19).
Aim: To describe the clinical aspects and outcomes of COVID-19 among KT recipients.
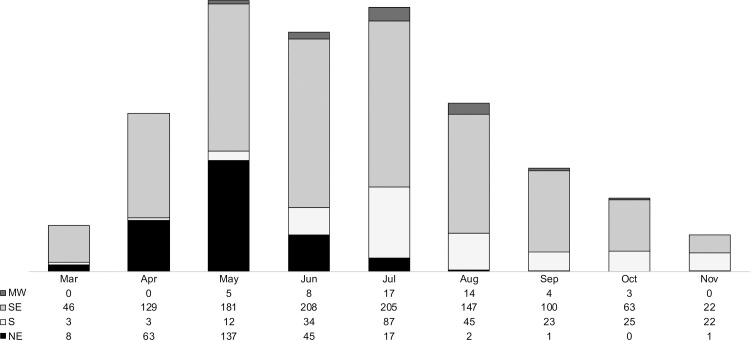
Methods: This multicenter cohort study enrolled 1,680 KT recipients diagnosed with COVID-19 between March and November 2020, from 35 Brazilian centers. The main outcome was the 90-day cumulative incidence of death, for the entire cohort and according to acute kidney injury (AKI) and renal replacement therapy (RRT) requirement. Fatality rates were analyzed according to hospitalization, intensive care unit (ICU) admission, and mechanical ventilation (MV) requirement. Multivariable analysis was performed by logistic regression for the probability of hospitalization and death.
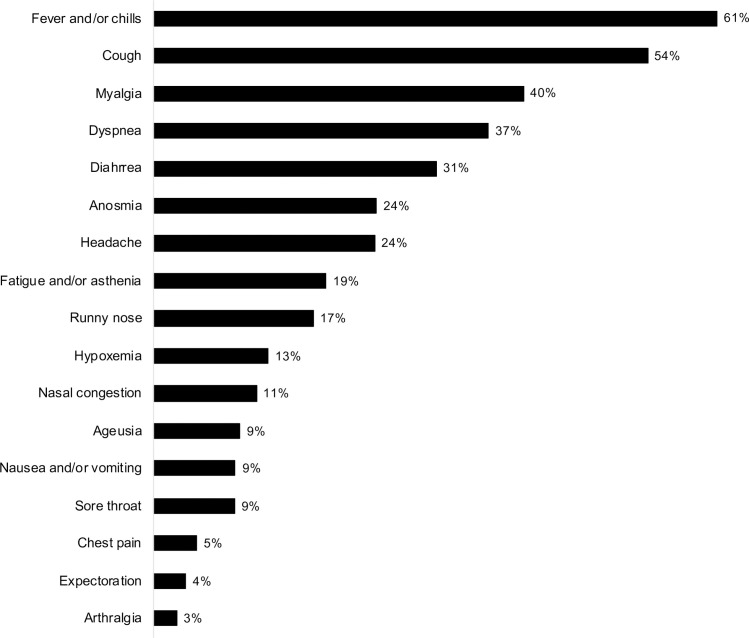
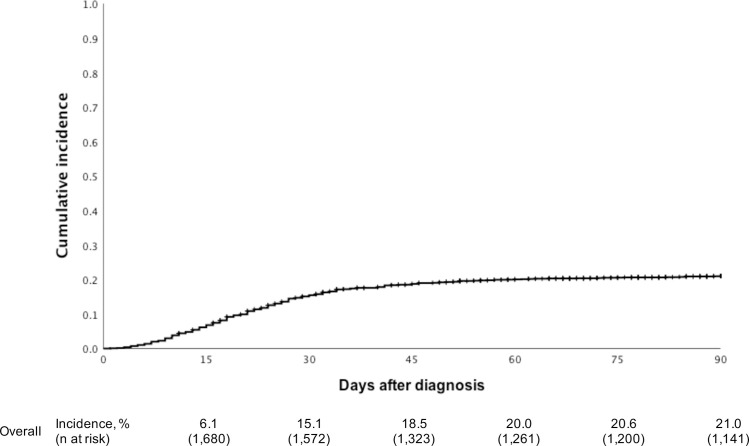
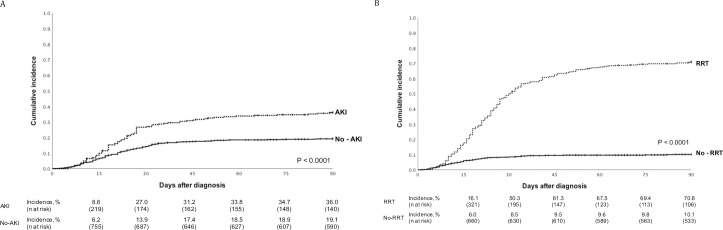
Results: The median age of the recipients was 51.3 years, 60.4% were men and 11.4% were Afro-Brazilian. Comorbidities were reported in 1,489 (88.6%), and the interval between transplantation and infection was 5.9 years. The most frequent symptoms were cough (54%), myalgia (40%), dyspnea (37%), and diarrhea (31%), whereas the clinical signs were fever (61%) and hypoxemia (13%). Hospitalization was required in 65.1%, and immunosuppressive drugs adjustments were made in 74.4% of in-hospital patients. ICU admission was required in 34.6% and MV in 24.9%. In the multivariable modeling, the variables related with the probability of hospitalization were age, hypertension, previous cardiovascular disease, recent use of high dose of steroid, and fever, dyspnea, diarrhea, and nausea or vomiting as COVID-19 symptoms. On the other hand, the variables that reduced the probability of hospitalization were time of COVID-19 symptoms, and nasal congestion, headache, arthralgia and anosmia as COVID-19 symptoms. The overall 90-day cumulative incidence of death was 21.0%. The fatality rates were 31.6%, 58.2%, and 75.5% in those who were hospitalized, admitted to the ICU, and required MV, respectively. At the time of infection, 23.2% had AKI and 23.4% required RRT in the follow-up. The cumulative incidence of death was significantly higher among recipients with AKI (36.0% vs. 19.1%, P < 0.0001) and in those who required RRT (70.8% vs. 10.1%, P < 0.0001). The variables related with the probability of death within 90 days after COVID-19 were age, time after transplantation, presence of hypertension, previous cardiovascular disease, use of tacrolimus and mycophenolate, recent use of high dose of steroids, and dyspnea as COVID-19 symptom. On the other hand, the variables that reduced the risk of death were time of symptoms, and headache and anosmia as COVID-19 symptoms.
Conclusion: The patients diagnosed with COVID-19 were long-term KT recipients and most of them had some comorbidities. One in every five patients died, and the rate of death was significantly higher in those with AKI, mainly when RRT was required.
Conflict of interest statement
The present study was partially supported by Novartis Pharma Brazil. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Brasil Coronavírus [Internet]. Available: https://covid.saude.gov.br/. [Accessed 2021 Feb 1].
-
- Sun K, Wang W, Gao L, Wang Y, Luo K, Ren L, et al.. Transmission heterogeneities, kinetics, and controllability of SARS-CoV-2. Science. 2021. Jan 15 [Cited 2021 Feb 1];371(6526). Available: https://science.sciencemag.org/content/371/6526/eabe2424. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
