

Influence of angiotensin converting enzyme inhibitors/angiotensin receptor blockers on the risk of all-cause mortality and other clinical outcomes in patients with confirmed COVID-19: A systemic review and meta-analysis
- PMID: 34320275
- PMCID: PMC8420264
- DOI: 10.1111/jch.14329
Influence of angiotensin converting enzyme inhibitors/angiotensin receptor blockers on the risk of all-cause mortality and other clinical outcomes in patients with confirmed COVID-19: A systemic review and meta-analysis
Abstract
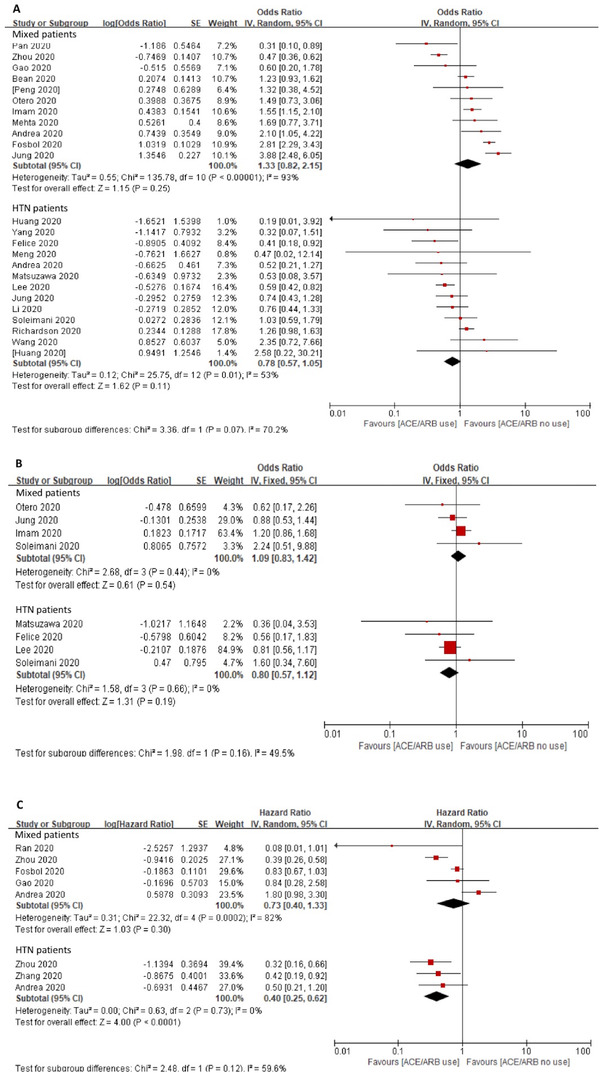
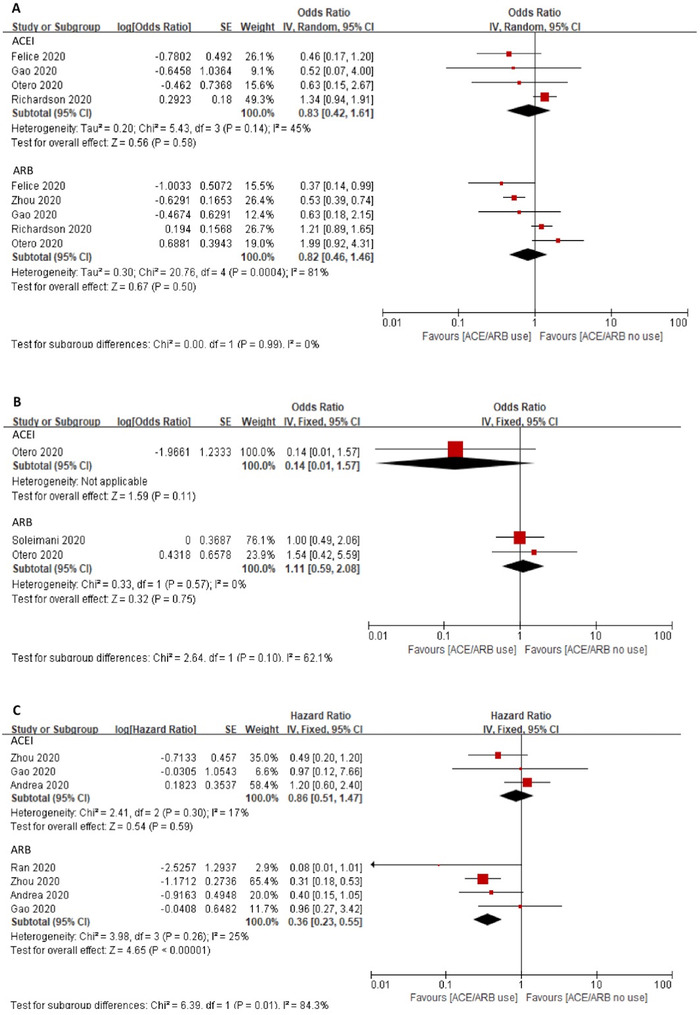
Since the COVID-19 pandemic, physicians concerned about the potential adverse effects of angiotensin converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs). To explore the relationship between ACEIs/ARBs and the risk of mortality and other clinical outcomes in COVID-19 patients, the authors conducted a systemic review and meta-analysis. An electronic search was performed from inception to November 12, 2020 in PubMed, Medline, EMBASE, ClinicalTrials, TRIP, the Cochrane Library, CNKI, Wanfang, and CBM database. Risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions tool. The primary outcome was in-hospital all-cause mortality. Secondary outcomes included all-cause mortality measured at 30-day or longer term, mechanical ventilation, length of hospital stay, readmission, and cardiac adverse events. A total of 28 studies with 73 465 patients was included. Twenty-two studies with 19 871 patients reported the incidence of all-cause mortality. Results showed no association between using ACEIs/ARBs and risk of mortality crude odds ratio (OR) of 1.02, 95% CI 0.71-1.46, p = .90, I2 = 88%, adjusted OR in 6260 patients of 0.96, 95% CI 0.77-1.18, p = .68, I2 = 0%. While six studies with 10 030 patients reported a lower risk of mortality in ACEIs/ARBs group hazard ratio (HR) of 0.53, 95% CI 0.34-0.84, p = .007, I2 = 68%. Similar association (for HR) was found in hypertension subgroup. There was no significant association for the secondary outcomes. Based on the available data, we concluded that ACEIs/ARBs is not associated with the risk of in-hospital all-cause mortality in COVID-19 patients, but may be associated with a decreased risk of 30-day all-cause mortality. Patients with hypertension may benefit from using ACEIs/ARBs.
Keywords: COVID-19; angiotensin converting enzyme inhibitor; angiotensin receptor blocker; mortality.
© 2021 The Authors. The Journal of Clinical Hypertension published by Wiley Periodicals LLC.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures


Comment in
-
Temporal variation, socioeconomic status, and out-of-hospital deaths as factors that influence mortality rates among hospitalized COVID-19 patients receiving ACEIs/ARBs.J Clin Hypertens (Greenwich). 2022 Apr;24(4):519-520. doi: 10.1111/jch.14473. Epub 2022 Mar 21. J Clin Hypertens (Greenwich). 2022. PMID: 35312155 Free PMC article. No abstract available.
-
Impact of more variations on in-hospital mortality among patients with confirmed COVID-19.J Clin Hypertens (Greenwich). 2022 Apr;24(4):521-522. doi: 10.1111/jch.14472. Epub 2022 Mar 21. J Clin Hypertens (Greenwich). 2022. PMID: 35312236 Free PMC article. No abstract available.
Similar articles
-
A systematic review and meta-analysis of the use of renin-angiotensin system drugs and COVID-19 clinical outcomes: What is the evidence so far?Pharmacol Res Perspect. 2020 Dec;8(6):e00666. doi: 10.1002/prp2.666. Pharmacol Res Perspect. 2020. PMID: 33084232 Free PMC article.
-
Association Between Renin-Angiotensin-Aldosterone System Inhibitors and Clinical Outcomes in Patients With COVID-19: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Mar 1;4(3):e213594. doi: 10.1001/jamanetworkopen.2021.3594. JAMA Netw Open. 2021. PMID: 33787911 Free PMC article.
-
A Retrospective Study from 2 Centers in China on the Effects of Continued Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in Patients with Hypertension and COVID-19.Med Sci Monit. 2020 Sep 24;26:e926651. doi: 10.12659/MSM.926651. Med Sci Monit. 2020. PMID: 32969367 Free PMC article.
-
Impact of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers on in-hospital mortality among patients with COVID-19: a systematic review and meta-analysis.Singapore Med J. 2021 Nov;62(11):563-567. doi: 10.11622/smedj.2020159. Epub 2020 Nov 30. Singapore Med J. 2021. PMID: 33256355 Free PMC article.
-
Angiotensin Converting Enzyme Inhibitors and Angiotensin Receptor Blockers and Mortality Among COVID-19 Patients: A Systematic Review and Meta-Analysis.Am J Ther. 2023 Jul-Aug 01;30(4):e336-e346. doi: 10.1097/MJT.0000000000001281. Epub 2020 Nov 10. Am J Ther. 2023. PMID: 33201001
Cited by
-
Renin-Angiotensin Aldosterone System Inhibitors and COVID-19: A Systematic Review and Meta-Analysis Revealing Critical Bias Across a Body of Observational Research.J Am Heart Assoc. 2022 Jun 7;11(11):e025289. doi: 10.1161/JAHA.122.025289. Epub 2022 May 27. J Am Heart Assoc. 2022. PMID: 35624081 Free PMC article.
-
Drug-Disease Severity and Target-Disease Severity Interaction Networks in COVID-19 Patients.Pharmaceutics. 2022 Aug 30;14(9):1828. doi: 10.3390/pharmaceutics14091828. Pharmaceutics. 2022. PMID: 36145576 Free PMC article.
-
Clinical Outcomes of Angiotensin Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers in COVID-19 Patients With Pre-existing Cardiac Comorbidities: A Literature Review.Cureus. 2023 Dec 28;15(12):e51244. doi: 10.7759/cureus.51244. eCollection 2023 Dec. Cureus. 2023. PMID: 38283421 Free PMC article. Review.
-
Temporal variation, socioeconomic status, and out-of-hospital deaths as factors that influence mortality rates among hospitalized COVID-19 patients receiving ACEIs/ARBs.J Clin Hypertens (Greenwich). 2022 Apr;24(4):519-520. doi: 10.1111/jch.14473. Epub 2022 Mar 21. J Clin Hypertens (Greenwich). 2022. PMID: 35312155 Free PMC article. No abstract available.
-
Cardiovascular Disease Complicating COVID-19 in the Elderly.Medicina (Kaunas). 2021 Aug 17;57(8):833. doi: 10.3390/medicina57080833. Medicina (Kaunas). 2021. PMID: 34441038 Free PMC article. Review.
References
-
- Cardiology CoHotESo . Position statement of the ESC Council on Hypertension on ACE‐inhibitors and angiotensin receptor blockers 2020. https://www.escardio.org/Councils/Council‐on‐Hypertension‐(CHT)/News/pos...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
