

Morphological Lesion Types Are Associated with Primary and Secondary Patency Rates after High-Pressure Balloon Angioplasty for Dysfunctional Arteriovenous Fistulas
- PMID: 34320498
- PMCID: PMC9153343
- DOI: 10.1159/000516883
Morphological Lesion Types Are Associated with Primary and Secondary Patency Rates after High-Pressure Balloon Angioplasty for Dysfunctional Arteriovenous Fistulas
Abstract
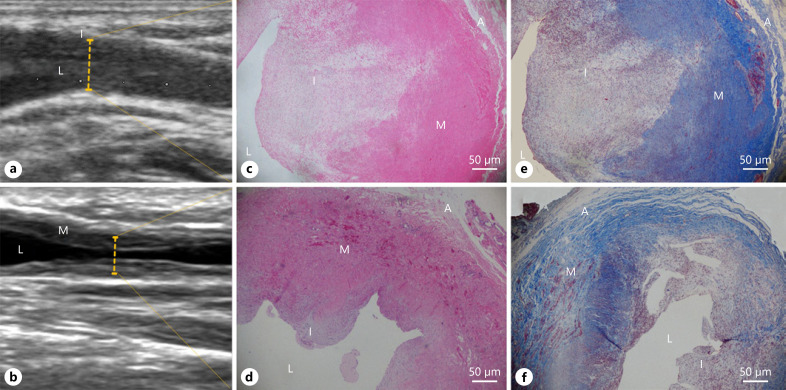
Background: Neointimal hyperplasia (NIH) is believed to be the main reason for arteriovenous fistula (AVF) dysfunction, but other mechanisms are also recognized to be involved in the pathophysiological process. This study investigated whether different morphological types of AVF lesions are associated with the patency rate after percutaneous transluminal angioplasty (PTA).
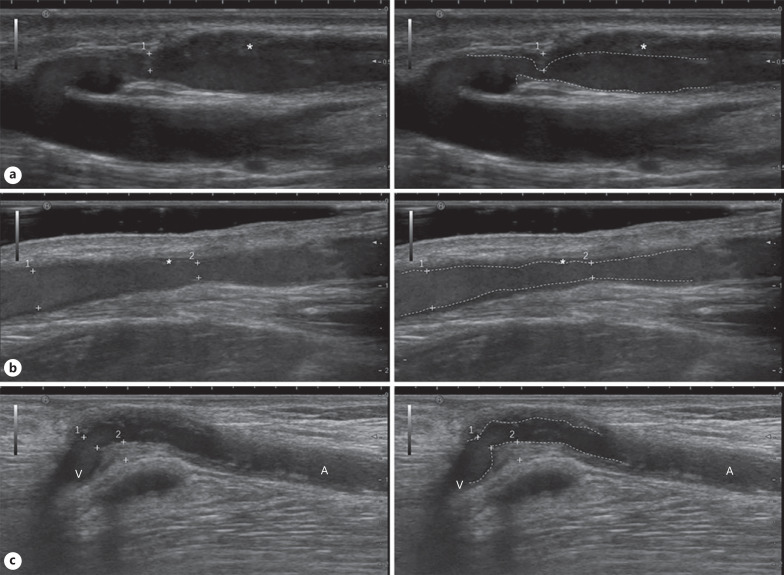
Methods: This retrospective study included 120 patients who underwent PTA for autogenous AVF dysfunction. All the cases were evaluated under Doppler ultrasound (DU) before intervention and divided into 3 types: Type I (NIH type), Type II (non-NIH type), and Type III (mixed type). Prognostic and clinical data were analyzed by Kaplan-Meier analysis and the Cox proportional hazards model.
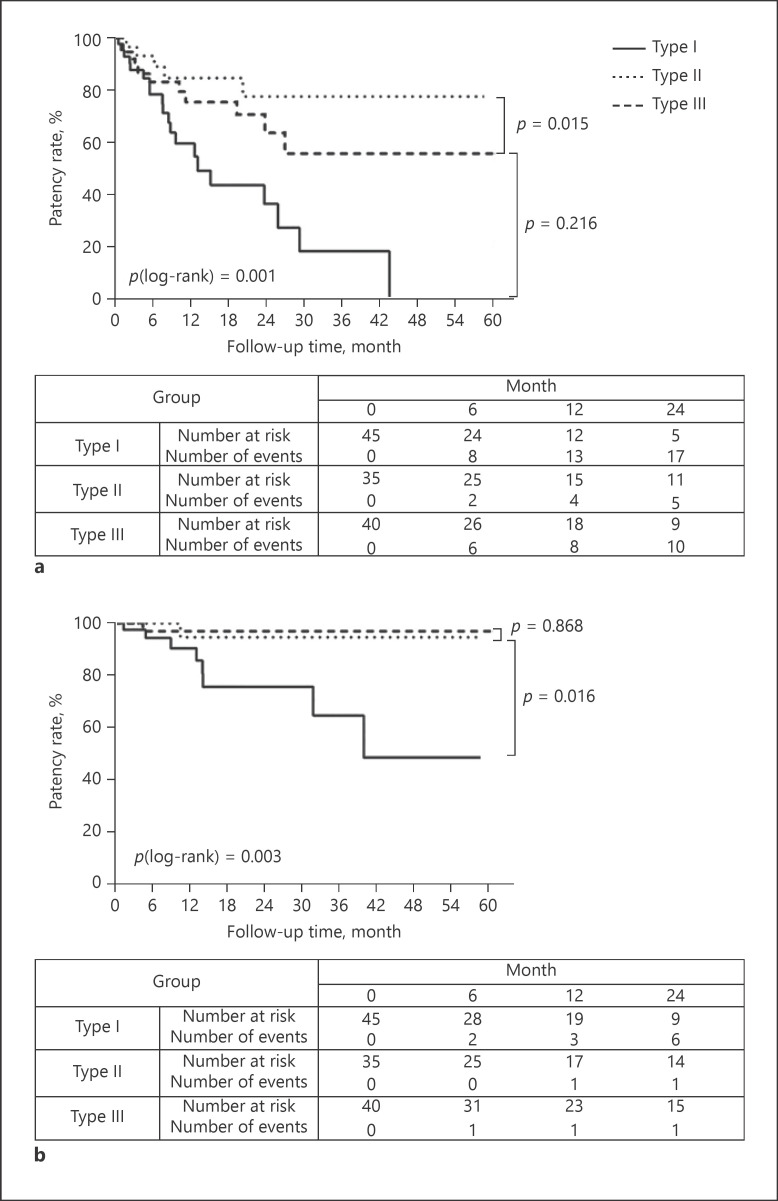
Results: There was no statistical difference in baseline variables among groups, except for lumen diameter. The primary patency rates in Type I, Type II, and Type III groups were 78.4, 93.2, and 83.2% at 6 months and 59.5, 84.7, and 75.5% at 1 year, respectively. The secondary patency rates in Type I, Type II, and Type III groups were 94.4, 97.1, and 100% at 6 months and 90.5, 97.1, and 94.7% at 1 year, respectively. The Kaplan-Meier curve showed that the primary and secondary patency rates of Type I group were lower than those of Type II group. Multivariable Cox regression analysis demonstrated that postoperative primary patency was correlated with end-to-end anastomosis (hazard ratio [HR] = 2.997, p = 0.008, 95% confidence interval [CI]: 1.328-6.764) and Type I lesion (HR = 5.395, p = 0.004, 95% CI: 1.730-16.824).
Conclusions: NIH-dominant lesions of AVF evaluated by DU preoperatively were a risk factor for poor primary and secondary patency rate after PTA in hemodialysis patients.
Keywords: Arteriovenous fistula dysfunction; Hemodialysis; Morphological type; Neointimal hyperplasia; Patency rate.
© 2021 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors declare that they have no relevant financial interests.
Figures
Similar articles
-
Factors affecting the primary patency of native arteriovenous fistulas after ultrasound-guided percutaneous transluminal angioplasty.Ren Fail. 2023 Dec;45(1):2233623. doi: 10.1080/0886022X.2023.2233623. Ren Fail. 2023. PMID: 37488970 Free PMC article.
-
Randomized clinical trial of cutting balloon angioplasty versus high-pressure balloon angioplasty in hemodialysis arteriovenous fistula stenoses resistant to conventional balloon angioplasty.J Vasc Interv Radiol. 2014 Feb;25(2):190-8. doi: 10.1016/j.jvir.2013.10.020. Epub 2013 Dec 5. J Vasc Interv Radiol. 2014. PMID: 24315548 Clinical Trial.
-
Impact of Lesion Morphology on Durability After Angioplasty of Failed Arteriovenous Fistulas in Hemodialysis Patients.J Endovasc Ther. 2018 Oct;25(5):649-654. doi: 10.1177/1526602817748316. Epub 2017 Dec 18. J Endovasc Ther. 2018. PMID: 29254461
-
Arteriovenous fistula aneurysmorrhaphy is associated with improved patency and decreased vascular access abandonment.J Vasc Surg. 2023 Mar;77(3):891-898.e1. doi: 10.1016/j.jvs.2022.10.054. Epub 2022 Nov 8. J Vasc Surg. 2023. PMID: 36368647 Review.
-
A systematic review and meta-analysis of the risk of death and patency after application of paclitaxel-coated balloons in the hemodialysis access.J Vasc Surg. 2020 Dec;72(6):2186-2196.e3. doi: 10.1016/j.jvs.2020.04.525. Epub 2020 Jun 12. J Vasc Surg. 2020. PMID: 32540324
Cited by
-
Comparison of ultrasound features and lesion sites in dysfunctional arteriovenous fistula.Ren Fail. 2024 Dec;46(1):2294148. doi: 10.1080/0886022X.2023.2294148. Epub 2024 Jan 8. Ren Fail. 2024. PMID: 38186351 Free PMC article.
-
Long-Term Efficacy of Ultrasound-Guided Percutaneous Transluminal Angioplasty for Arteriovenous Fistula Outflow Stenosis Caused by Venous Valve.Kidney Dis (Basel). 2024 Jan 24;10(2):89-96. doi: 10.1159/000536309. eCollection 2024 Apr. Kidney Dis (Basel). 2024. PMID: 38751797 Free PMC article.
-
Factors affecting the primary patency of native arteriovenous fistulas after ultrasound-guided percutaneous transluminal angioplasty.Ren Fail. 2023 Dec;45(1):2233623. doi: 10.1080/0886022X.2023.2233623. Ren Fail. 2023. PMID: 37488970 Free PMC article.
-
Comparison of the primary outcome of the radial artery deviation and reimplantation technique and the ultrasound-guided percutaneous transluminal angioplasty in the treatment of forearm arteriovenous fistula type I stenosis in haemodialysis patients: a pilot study.Int Urol Nephrol. 2025 Jun 13. doi: 10.1007/s11255-025-04614-y. Online ahead of print. Int Urol Nephrol. 2025. PMID: 40512328
References
-
- Zhang L, Zuo L. Current burden of end-stage kidney disease and its future trend in China. Clin Nephrol. 2016;86((13)):27–8. - PubMed
-
- Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, et al. KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis. 2020;75((4Suppl 2)):S1–164. - PubMed
-
- Rothuizen TC, Wong C, Quax PH, van Zonneveld AJ, Rabelink TJ, Rotmans JI. Arteriovenous access failure: more than just intimal hyperplasia? Nephrol Dial Transplant. 2013;28((5)):1085–92. - PubMed
-
- Roy-Chaudhury P, Sukhatme VP, Cheung AK. Hemodialysis vascular access dysfunction: a cellular and molecular viewpoint. J Am Soc Nephrol. 2006;17((4)):1112–27. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
