

Renin-Angiotensin Aldosterone System Inhibitors in Primary Prevention and COVID-19
- PMID: 34320843
- PMCID: PMC8475700
- DOI: 10.1161/JAHA.120.021154
Renin-Angiotensin Aldosterone System Inhibitors in Primary Prevention and COVID-19
Abstract
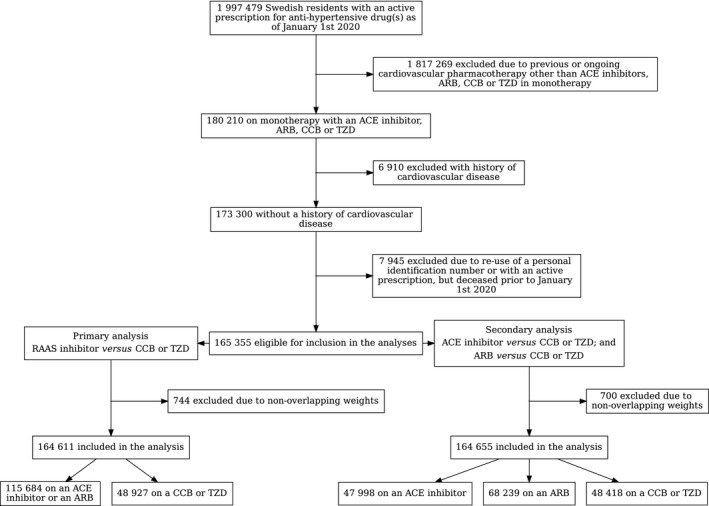
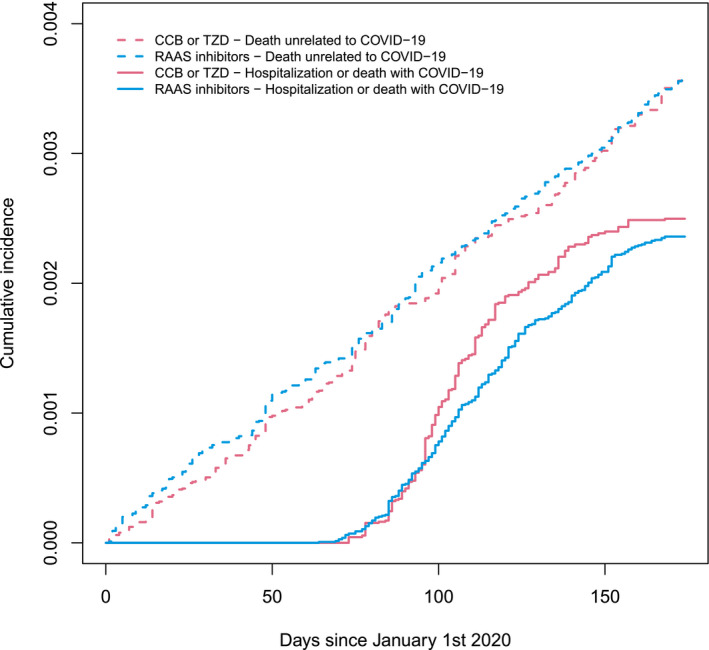
Background Considering the widespread risk of collider bias and confounding by indication in previous research, the associations between renin-angiotensin aldosterone system (RAAS) inhibitor use and COVID-19 remain unknown. Accordingly, this study tested the hypothesis that RAAS inhibitors influence the summation effect of COVID-19 and its progression to severe outcomes. Methods and Results This nationwide cohort study compared all residents of Sweden, without prior cardiovascular disease, in monotherapy (as of January 1, 2020) with a RAAS inhibitor to those using a calcium channel blocker or a thiazide diuretic. Comparative cohorts were balanced using machine-learning-derived propensity score methods. Of 165 355 people in the analysis (51% women), 367 were hospitalized or died with COVID-19 (246 using a RAAS inhibitor versus 121 using a calcium channel blocker or thiazide diuretic; Cox proportional hazard ratio [HR], 0.97; 95% CI, 0.74-1.27). When each outcome was assessed separately, 335 people were hospitalized with COVID-19 (HR, 0.92; 95% CI, 0.70-1.22), and 64 died with COVID-19 (HR, 1.22; 95% CI, 0.68-2.19). The severity of COVID-19 outcomes did not differ between those using a RAAS inhibitor and those using a calcium channel blocker or thiazide diuretic (ordered logistic regression odds ratio, 1.01; 95% CI, 0.89-1.14). Conclusions Despite potential limitations, this study is among the best available evidence that RAAS inhibitor use in primary prevention does not increase the risk of severe COVID-19 outcomes; presenting strong data from which scientists and policy makers alike can base, with greater confidence, their current position on the safety of using RAAS inhibitors during the COVID-19 pandemic.
Keywords: COVID‐19; SARS‐CoV‐2; angiotensin II receptor blocker; angiotensin‐converting enzyme inhibitor; hypertension.
Conflict of interest statement
None.
Figures
Similar articles
-
Renin-Angiotensin Aldosterone System Inhibitors and COVID-19: A Systematic Review and Meta-Analysis Revealing Critical Bias Across a Body of Observational Research.J Am Heart Assoc. 2022 Jun 7;11(11):e025289. doi: 10.1161/JAHA.122.025289. Epub 2022 May 27. J Am Heart Assoc. 2022. PMID: 35624081 Free PMC article.
-
Resistant Hypertension On Treatment (ResHypOT): sequential nephron blockade compared to dual blockade of the renin-angiotensin-aldosterone system plus bisoprolol in the treatment of resistant arterial hypertension - study protocol for a randomized controlled trial.Trials. 2018 Feb 12;19(1):101. doi: 10.1186/s13063-017-2343-3. Trials. 2018. PMID: 29433578 Free PMC article.
-
Comparison of renin-angiotensin-aldosterone system inhibitors with other antihypertensives in association with coronavirus disease-19 clinical outcomes.BMC Infect Dis. 2021 Jun 5;21(1):527. doi: 10.1186/s12879-021-06088-6. BMC Infect Dis. 2021. PMID: 34090358 Free PMC article.
-
Influence of blood pressure control and application of renin-angiotensin-aldosterone system inhibitors on the outcomes in COVID-19 patients with hypertension.J Clin Hypertens (Greenwich). 2020 Nov;22(11):1974-1983. doi: 10.1111/jch.14038. Epub 2020 Oct 2. J Clin Hypertens (Greenwich). 2020. PMID: 33006442 Free PMC article.
-
Renin-angiotensin-aldosterone system inhibitors and the risk of mortality in patients with hypertension hospitalised for COVID-19: systematic review and meta-analysis.Open Heart. 2020 Nov;7(2):e001353. doi: 10.1136/openhrt-2020-001353. Open Heart. 2020. PMID: 33154144 Free PMC article.
Cited by
-
Inflammation and vascular dysfunction: The negative synergistic combination of diabetes and COVID-19.Diabetes Metab Res Rev. 2022 Oct;38(7):e3565. doi: 10.1002/dmrr.3565. Epub 2022 Jul 22. Diabetes Metab Res Rev. 2022. PMID: 35830597 Free PMC article. Review.
-
Initiation of antihypertensive drugs to patients with confirmed COVID-19-A population-based cohort study in Sweden.Basic Clin Pharmacol Toxicol. 2022 Sep;131(3):196-204. doi: 10.1111/bcpt.13766. Epub 2022 Jul 6. Basic Clin Pharmacol Toxicol. 2022. PMID: 35726121 Free PMC article.
-
Cardiovascular Disease Complicating COVID-19 in the Elderly.Medicina (Kaunas). 2021 Aug 17;57(8):833. doi: 10.3390/medicina57080833. Medicina (Kaunas). 2021. PMID: 34441038 Free PMC article. Review.
-
Angiotensin II infusion in COVID-19: An international, multicenter, registry-based study.J Med Virol. 2022 May;94(5):2079-2088. doi: 10.1002/jmv.27592. Epub 2022 Jan 21. J Med Virol. 2022. PMID: 35029318 Free PMC article.
-
Impact of the COVID-19 pandemic on initiation of antihypertensive drugs in Sweden: an interrupted time series study.BMJ Open. 2024 Oct 16;14(10):e082209. doi: 10.1136/bmjopen-2023-082209. BMJ Open. 2024. PMID: 39414273 Free PMC article.
References
-
- Hoffmann M, Kleine‐Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu N‐H, Nitsche A, et al. SARS‐CoV‐2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–280.e8. DOI: 10.1016/j.cell.2020.02.052. - DOI - PMC - PubMed
-
- Ferrario CM, Jessup J, Chappell MC, Averill DB, Brosnihan KB, Tallant EA, Diz DI, Gallagher PE. Effect of angiotensin‐converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin‐converting enzyme 2. Circulation. 2005;111:2605–2610. DOI: 10.1161/CIRCULATIONAHA.104.510461. - DOI - PubMed
-
- Adrish M, Chilimuri S, Sun H, Mantri N, Yugay A, Zahid M. The association of renin‐angiotensin‐aldosterone system inhibitors with outcomes among a predominantly ethnic minority patient population hospitalized with COVID‐19: the Bronx experience. Cureus. 2020;12:e10217. DOI: 10.7759/cureus.10217. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
