

Chronic respiratory disease disparity between American Indian/Alaska Native and white populations, 2011-2018
- PMID: 34320979
- PMCID: PMC8317382
- DOI: 10.1186/s12889-021-11528-8
Chronic respiratory disease disparity between American Indian/Alaska Native and white populations, 2011-2018
Abstract
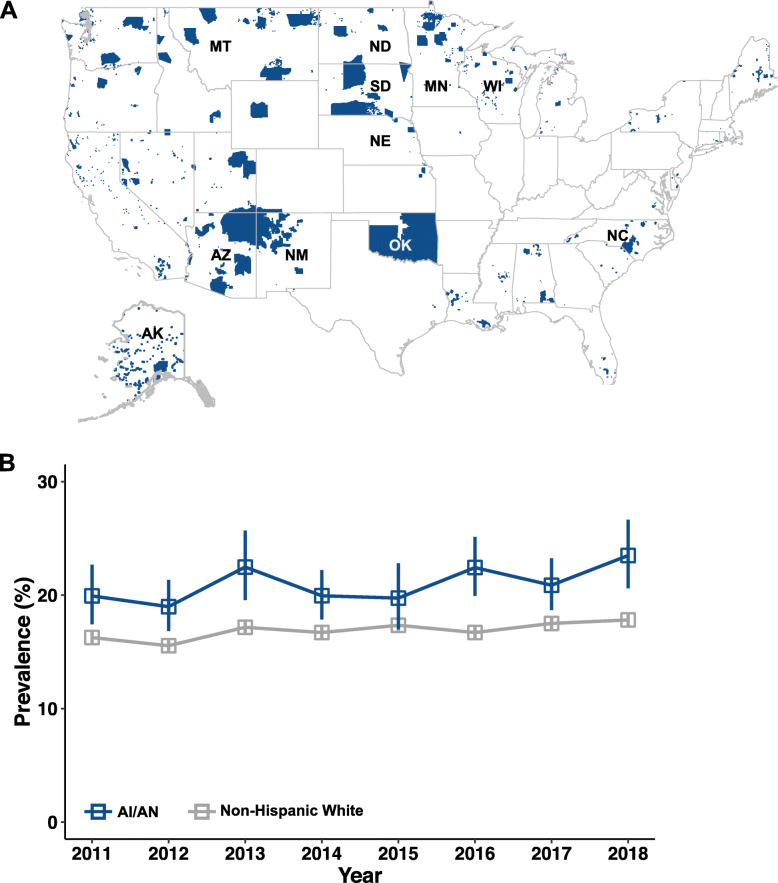
Background: American Indian/Alaska Native (AI/AN) populations have been disproportionately affected by chronic respiratory diseases for reasons incompletely understood. Past research into disease disparity using population-based surveys mostly focused on state-specific factors. The present study investigates the independent contributions of AI/AN racial status and other socioeconomic/demographic variables to chronic respiratory disease disparity in an 11-state region with historically high AI/AN representation. Using data from the Behavioral Risk Factor Surveillance System (BRFSS) spanning years 2011-2018, this work provides an updated assessment of disease disparity and potential determinants of respiratory health in AI/AN populations.
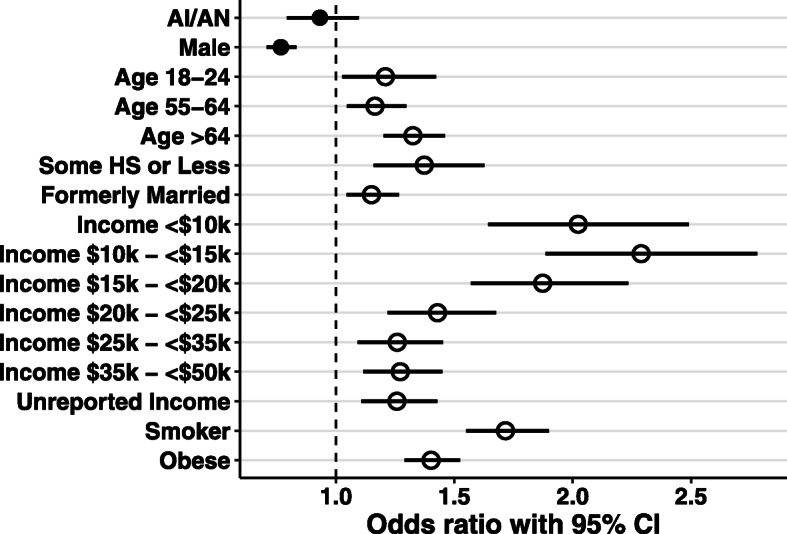
Methods: This cross-sectional study used data from the BRFSS survey, 2011-2018. The study population included AI/AN and non-Hispanic white individuals resident in 11 states with increased proportion of AI/AN individuals. The yearly number of respondents averaged 75,029 (62878-87,350) which included approximately 5% AI/AN respondents (4.5-6.3%). We compared the yearly adjusted prevalence for chronic respiratory disease, where disease status was defined by self-reported history of having asthma and/or chronic obstructive pulmonary disease (COPD). Multivariable logistic regression was performed to determine if being AI/AN was independently associated with chronic respiratory disease. Covariates included demographic (age, sex), socioeconomic (marital status, education level, annual household income), and behavioral (smoking, weight morbidity) variables.
Results: The AI/AN population consistently displayed higher adjusted prevalence of chronic respiratory disease compared to the non-Hispanic white population. However, the AI/AN race/ethnicity characteristic was not independently associated with chronic respiratory disease (OR, 0.93; 95% CI, 0.79-1.10 in 2017). In contrast, indicators of low socioeconomic status such as annual household income of <$10,000 (OR, 2.02; 95% CI, 1.64-2.49 in 2017) and having less than high school education (OR, 1.37; 95% CI, 1.16-1.63 in 2017) were positively associated with disease. These trends persisted for all years analyzed.
Conclusions: This study highlighted that AI/AN socioeconomic burdens are key determinants of chronic respiratory disease, in addition to well-established risk factors such as smoking and weight morbidity. Disease disparity experienced by the AI/AN population is therefore likely a symptom of disproportionate socioeconomic challenges they face. Further promotion of public health and social service efforts may be able to improve AI/AN health and decrease this disease disparity.
Keywords: American Indian/Alaskan Native; BRFSS; Chronic respiratory disease; Health disparities.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- National Asthma Education and Prevention Program . Expert panel report III: Guidelines for the diagnosis and management of asthma. Bethesda: National Heart, Lung, and Blood Institute; 2007.
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2020 Report. https://www.goldcopd.org. Accessed 28 Mar 2020. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
