

Cyclophosphamide for interstitial lung disease-associated acute respiratory failure: mortality, clinical response and radiological characteristics
- PMID: 34320981
- PMCID: PMC8316896
- DOI: 10.1186/s12890-021-01615-2
Cyclophosphamide for interstitial lung disease-associated acute respiratory failure: mortality, clinical response and radiological characteristics
Abstract
Background: Treatment for interstitial lung disease (ILD) patients with acute respiratory failure (ARF) is challenging, and literature to guide such treatment is scarce. The reported in-hospital mortality rates of ILD patients with ARF are high (62-66%). Cyclophosphamide is considered a second-line treatment in steroid-refractory ILD-associated ARF. The first aim of this study was to evaluate the in-hospital mortality in patients with ILD-associated ARF treated with cyclophosphamide. The second aim was to compare computed tomographic (CT) patterns and physiological and ventilator parameters between survivors and non-survivors.
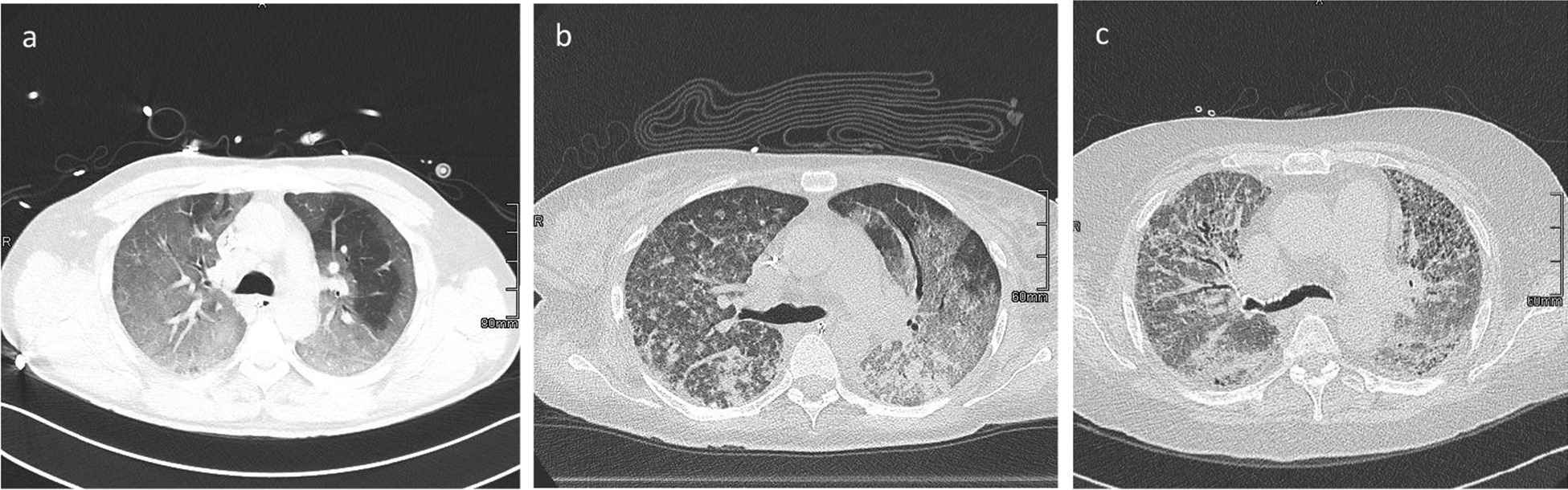
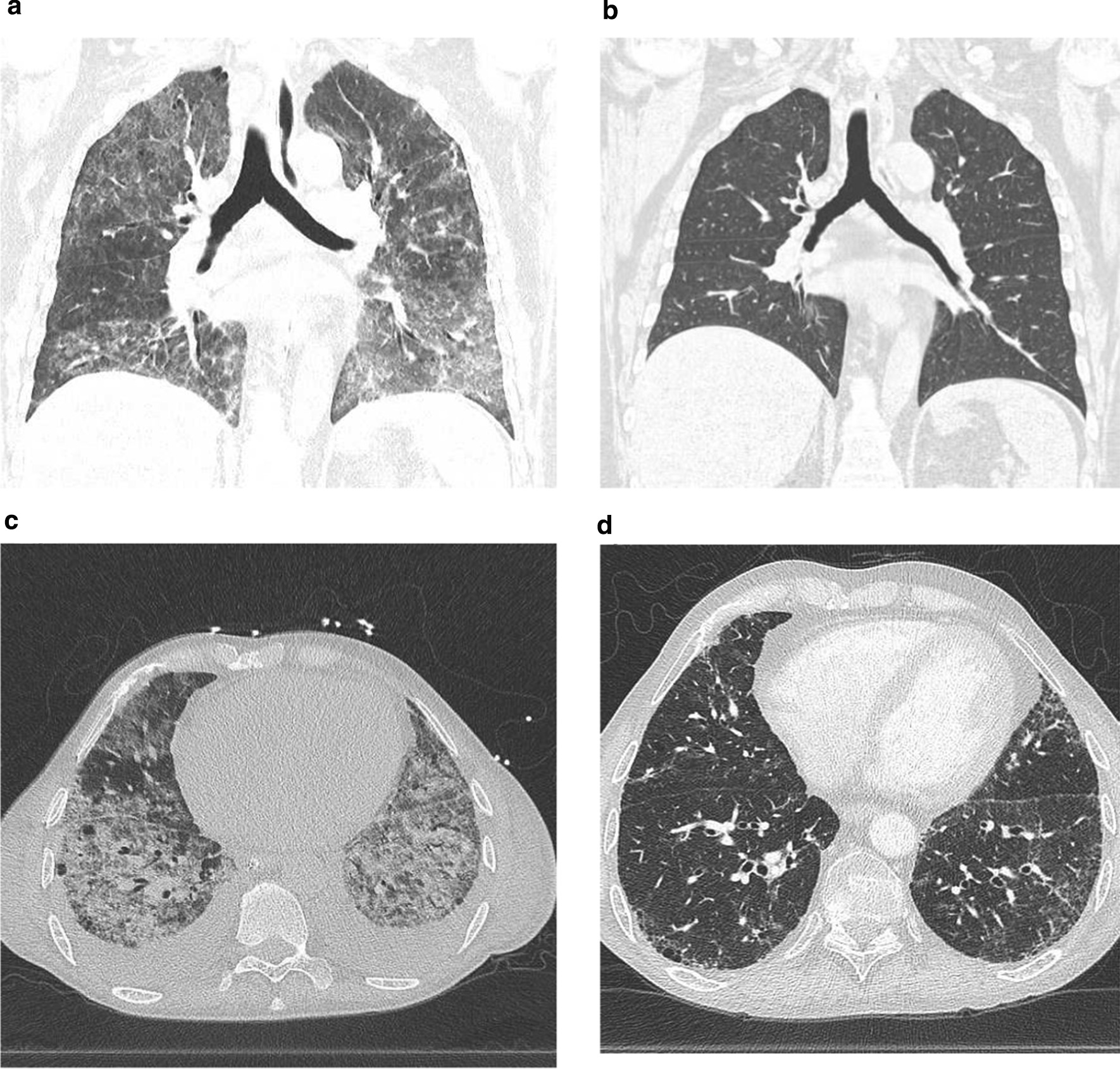
Methods: Retrospective analysis of patients with ILD-associated ARF treated with cyclophosphamide between February 2016 and October 2017. Patients were categorized into three subgroups: connective tissue disease (CTD)-associated ILD, other ILD or vasculitis. In-hospital mortality was evaluated in the whole cohort and in these subgroups. Clinical response was determined using physiological and ventilator parameters: Sequential Organ Failure Assessment Score (SOFA), PaO2/FiO2 (P/F) ratio and dynamic compliance (Cdyn) before and after cyclophosphamide treatment. The following CT features were quantified: ground-glass opacification (GGO) proportion, reticulation proportion, overall extent of parenchymal disease and fibrosis coarseness score.
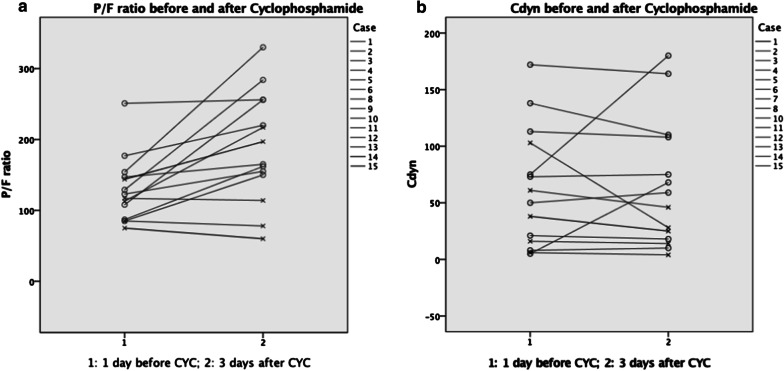
Results: Fifteen patients were included. The overall in-hospital mortality rate was 40%. In-hospital mortality rates for CTD-associated ILD, other ILD and vasculitis were 20, 57, and 33%, respectively. The GGO proportion (71% vs 45%) was higher in non-survivors. There were no significant differences in the SOFA score, P/F ratio or Cdyn between survivors and non-survivors. However, in survivors the P/F ratio increased from 129 to 220 mmHg and Cdyn from 75 to 92 mL/cmH2O 3 days after cyclophosphamide treatment. In non-survivors the P/F ratio hardly changed (113-114 mmHg) and Cdyn even decreased (27-20 mL/cmH2O).
Conclusion: In this study, we found a mortality rate of 40% in patients treated with cyclophosphamide for ILD-associated ARF. Connective tissue disease-associated ILD and vasculitis were associated with a lower risk of death. In non-survivors, the CT GGO proportion was significantly higher. The P/F ratio and Cdyn in survivors increased after 3 days of cyclophosphamide treatment.
Keywords: Acute respiratory failure; Cyclophosphamide; Ground-glass opacification; Interstitial lung disease.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Rituximab versus cyclophosphamide for the treatment of connective tissue disease-associated interstitial lung disease (RECITAL): study protocol for a randomised controlled trial.Trials. 2017 Jun 15;18(1):275. doi: 10.1186/s13063-017-2016-2. Trials. 2017. PMID: 28619061 Free PMC article. Clinical Trial.
-
Efficacy and safety of oral versus intravenous cyclophosphamide in treatment of connective tissue disease-related interstitial lung disease.Int J Rheum Dis. 2024 Oct;27(10):e15354. doi: 10.1111/1756-185X.15354. Int J Rheum Dis. 2024. PMID: 39352049
-
Intravenous cyclophosphamide pulse therapy in interstitial lung disease associated with systemic sclerosis in a retrospective open-label study: influence of the extent of inflammation on pulmonary function.Clin Rheumatol. 2018 Oct;37(10):2715-2722. doi: 10.1007/s10067-018-4171-6. Epub 2018 Jul 10. Clin Rheumatol. 2018. PMID: 29987427 Free PMC article.
-
Current and Emerging Drug Therapies for Connective Tissue Disease-Interstitial Lung Disease (CTD-ILD).Drugs. 2019 Sep;79(14):1511-1528. doi: 10.1007/s40265-019-01178-x. Drugs. 2019. PMID: 31399860 Review.
-
Review series: Aspects of interstitial lung disease: connective tissue disease-associated interstitial lung disease: how does it differ from IPF? How should the clinical approach differ?Chron Respir Dis. 2011;8(1):53-82. doi: 10.1177/1479972310393758. Chron Respir Dis. 2011. PMID: 21339375 Review.
Cited by
-
Network analysis-based strategy to investigate the protective effect of cepharanthine on rat acute respiratory distress syndrome.Front Pharmacol. 2022 Oct 26;13:1054339. doi: 10.3389/fphar.2022.1054339. eCollection 2022. Front Pharmacol. 2022. PMID: 36386130 Free PMC article.
References
-
- Vial-Dupuy A, Sanchez O, Douvry B, et al. Outcome of patients with interstitial lung disease admitted to the intensive care unit. Sarcoidosis Vasc Diffuse Lung Dis. 2013;30(2):134–142. - PubMed
-
- Wells AU, Hirani N, on behalf of the British Thoracic Society Interstitial Lung Disease Guideline Group, a subgroup of the British Thoracic Society Standards of CareCommittee, in collaboration with the Thoracic Society of Australia and New Zealandand the Irish Thoracic Society. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax. 2008;63;v1–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
