

Geometric changes in aortic root replacement using Freestyle prosthesis
- PMID: 34321027
- PMCID: PMC8320201
- DOI: 10.1186/s13019-021-01583-y
Geometric changes in aortic root replacement using Freestyle prosthesis
Abstract
Background: The Medtronic Freestyle prosthesis has proven to be a promising recourse for aortic root replacement in various indications. The present study aims to evaluate clinical outcomes and geometric changes of the aorta after Freestyle implantation.
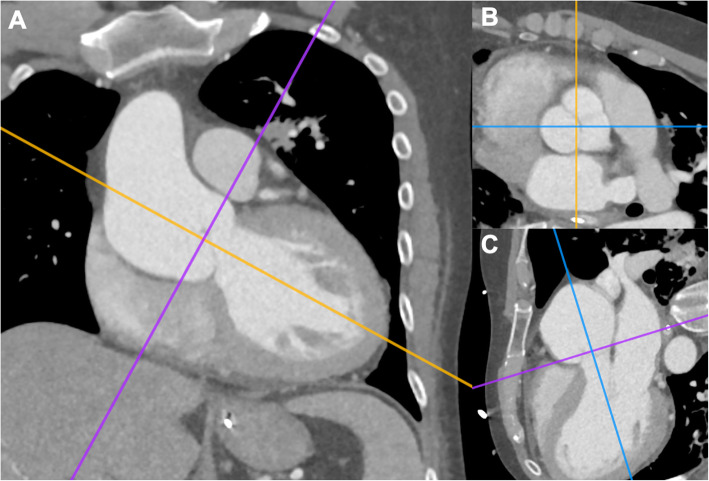
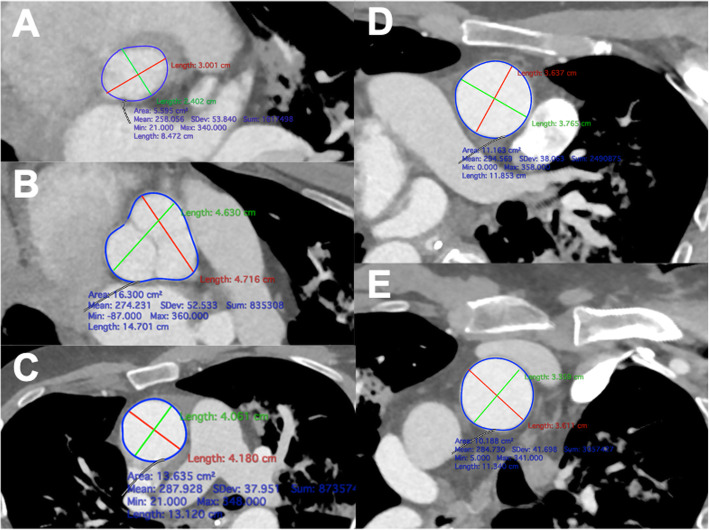
Methods: Between October 2005 and November 2020, the computed tomography angiography (CTA) data of 32 patients were analyzed in a cohort of 68 patients that underwent aortic root replacement using Freestyle prosthesis. The minimum and maximum diameters and areas of the aortic annulus, aortic root, ascending aorta, and the proximal aortic arch were measured at a plane perpendicular to the long axis of the aorta using 3D multiplanar reconstruction in both the preoperative (n = 32) and postoperative (n = 10) CTAs. Moreover, volumetric changes of the aortic root and ascending aorta were quantified.
Results: Mean age was 64.6 ± 10.6 years. Indications for surgery using Freestyle prosthesis were combined aortic valve pathologies, aortic aneurysm or dissection, and endocarditis, with concomitant surgery occurring in 28 out of 32 patients. In-hospital mortality was 18.6%. Preoperative diameter and area measurements of the aortic annulus strongly correlated with the implanted valve size (p < 0.001). Bicuspid valve was present in 28.1% of the patients. Diameter and areas of the aortic root decreased after freestyle implantation, resulting in a reduction of the aortic root volume (45.6 ± 26.3 cm3 to 18.7 ± 4.5 cm3, p = 0.029). Volume of the aortic root and the ascending aorta decreased from 137.3 ± 65.2 cm3 to 54.5 ± 21.1 cm3 after Freestyle implantation (p = 0.023).
Conclusion: Implantation of the Freestyle prosthesis presents excellent results in restoring the aortic geometry. Preoperative CTA measurements are beneficial to the surgical procedure and valve selection and therefore, if available, should be considered in pre-operative planning.
Keywords: Aortic root; Aortic valve replacement; Bioroot; Computed tomography measurement.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Root replacement with stentless Freestyle bioprostheses for active endocarditis: a single centre experience.Interact Cardiovasc Thorac Surg. 2013 Jan;16(1):27-30. doi: 10.1093/icvts/ivs438. Epub 2012 Oct 26. Interact Cardiovasc Thorac Surg. 2013. PMID: 23103719 Free PMC article.
-
Medtronic Freestyle aortic root bioprosthesis: Implant techniques.J Card Surg. 1998 Sep-Oct;13(5):369-75. doi: 10.1111/j.1540-8191.1998.tb01099.x. J Card Surg. 1998. PMID: 10440652 Clinical Trial.
-
Clinical Outcomes Using Freestyle Valve-Valsalva Graft Composite Conduit for Aortic Root Replacement.Ann Thorac Surg. 2022 Sep;114(3):643-649. doi: 10.1016/j.athoracsur.2021.12.022. Epub 2022 Jan 11. Ann Thorac Surg. 2022. PMID: 35031292 Review.
-
Long Term Outcomes of Freestyle Stentless Aortic Bioprosthesis: A Single Center Experience.Heart Surg Forum. 2020 Feb 10;23(1):E034-E038. doi: 10.1532/hsf.2661. Heart Surg Forum. 2020. PMID: 32118540
-
[Aortic root reconstruction in elderly patients].Kyobu Geka. 2005 Jul;58(8 Suppl):695-700. Kyobu Geka. 2005. PMID: 16097620 Review. Japanese.
References
-
- Cohen G, Zagorski B, Christakis GT, Joyner CD, Vincent J, Sever J, Harbi S, Feder-Elituv R, Moussa F, Goldman BS, Fremes SE. Are stentless valves hemodynamically superior to stented valves? Long-term follow-up of a randomized trial comparing Carpentier-Edwards pericardial valve with the Toronto Stentless porcine valve. J Thorac Cardiovasc Surg. 2010;139(4):848–859. doi: 10.1016/j.jtcvs.2009.04.067. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
