

Intensive care-treated cardiac arrest: a retrospective study on the impact of extended age on mortality, neurological outcome, received treatments and healthcare-associated costs
- PMID: 34321064
- PMCID: PMC8317381
- DOI: 10.1186/s13049-021-00923-0
Intensive care-treated cardiac arrest: a retrospective study on the impact of extended age on mortality, neurological outcome, received treatments and healthcare-associated costs
Abstract
Background: Cardiac arrest (CA) is a leading cause of death worldwide. As population ages, the need for research focusing on CA in elderly increases. This study investigated treatment intensity, 12-month neurological outcome, mortality and healthcare-associated costs for patients aged over 75 years treated for CA in an intensive care unit (ICU) of a tertiary hospital.
Methods: This single-centre retrospective study included adult CA patients treated in a Finnish tertiary hospital's ICU between 2005 and 2013. We stratified the study population into two age groups: <75 and [Formula: see text]75 years. We compared interventions defined by the median daily therapeutic scoring system (TISS-76) between the age groups to find differences in treatment intensity. We calculated cost-effectiveness by dividing the total one-year healthcare-associated costs of all patients by the number of survivors with a favourable neurological outcome. Favourable outcome was defined as a cerebral performance category (CPC) of 1-2 at 12 months after cardiac arrest. Logistic regression analysis was used to identify independent associations between age group, mortality and neurological outcome.
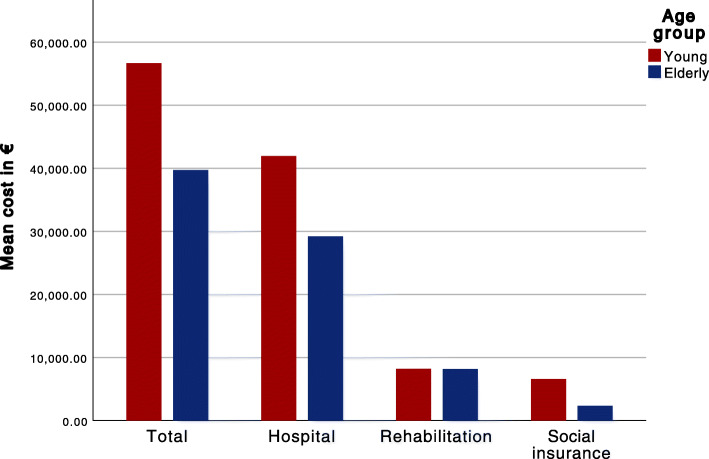
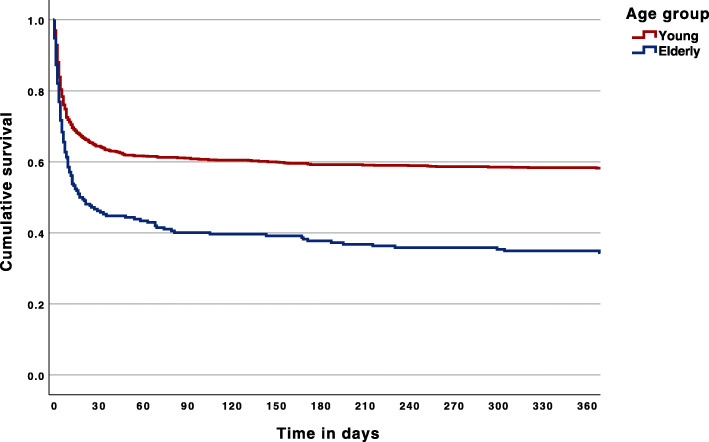
Results: This study included a total of 1,285 patients, of which 212 (16 %) were [Formula: see text]75 years of age. Treatment intensity was lower for the elderly compared to the younger group, with median TISS scores of 116 and 147, respectively (p < 0.001). The effective cost in euros for patients with a good one-year neurological outcome was €168,000 for the elderly and €120,000 for the younger group. At 12 months after CA 24 % of the patients in the elderly group and 47 % of the patients in the younger group had a CPC of 1-2 (p < 0.001). Age was an independent predictor of mortality (multivariate OR = 2.90, 95 % CI: 1.94-4.31, p < 0.001) and neurological outcome (multivariate OR = 3.15, 95 % CI: 2.04-4.86, p < 0.001).
Conclusions: The elderly ICU-treated CA patients in this study had worse neurological outcomes, higher mortality and lower cost-effectiveness than younger patients. Elderly received less intense treatment. Further efforts are needed to recognize the tools for assessing which elderly patients benefit from a more aggressive treatment approach in order to improve the cost-effectiveness of post-CA management.
Keywords: Cardiac arrest; Elderly; ICUCA; IHCA; OHCA; cardiopulmonary resuscitation; critical care; intensive care unit.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
