Changes in expression of PD-L1 on peripheral T cells in patients with melanoma and lung cancer treated with PD-1 inhibitors
- PMID: 34321489
- PMCID: PMC8319434
- DOI: 10.1038/s41598-021-93479-z
Changes in expression of PD-L1 on peripheral T cells in patients with melanoma and lung cancer treated with PD-1 inhibitors
Abstract
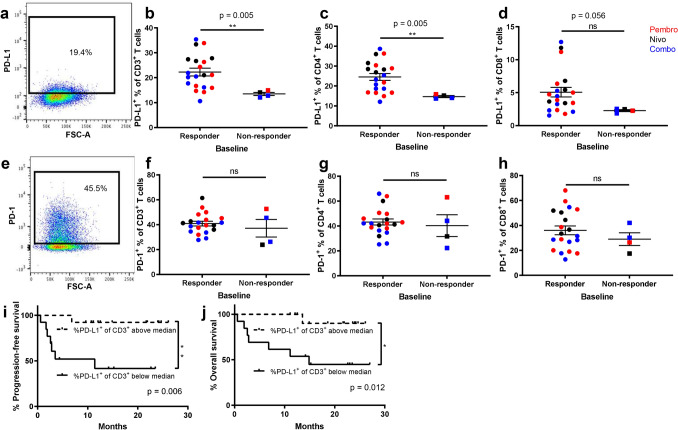
Advances in cancer immunology have increased the use of immune checkpoint inhibitors in clinical practice, however not all patients respond, and treatment can have severe side-effects. Blood-based immunological biomarkers are an attractive method for predicting which patients will respond to therapy, however, reliable biomarkers for immune checkpoint blockade are lacking. This study aimed to identify patients before or early in treatment who would best respond to PD-1 inhibitors. We hypothesised that higher baseline PD-L1 and/or PD-1 on peripheral blood T cells could predict radiological response to PD-1 inhibitors. This pilot prospective cohort study assessed 26 patients with melanoma or non-small cell lung cancer, treated with pembrolizumab, nivolumab, or nivolumab/ipilimumab combined. Response was assessed by RECIST 1.1. Peripheral blood lymphocytes collected at baseline, after one cycle, 10 weeks and at discontinuation of therapy were analysed by flow cytometry. Patients with a higher proportion of PD-L1+ T cells at baseline had improved objective response to PD-1 inhibitor therapy, and patients with a lower proportion of regulatory T cells at baseline experienced more immune-related adverse events. These findings may prove useful to assist in clinical decision making. Further studies with larger cohorts are required to validate these findings.
© 2021. The Author(s).
Conflict of interest statement
M.J.M. and T.M.M. declare serving on the advisory boards for AstraZeneca, Bristol-Myers Squibb, Merck Sharp & Dohme and Novartis. M.J.M. also declares serving on the advisory boards for Pfizer and Roche. M.J.M. and T.M.M. declare receiving travel support from AstraZeneca, Bristol-Meyers Squibb and Roche. S.J.D., A.M.C., A.M.M., W.L.C, M.U.H. and S.E.B. declare they have no competing interests related to the work described.
Figures