

Proof of concept study to develop a novel connectivity-based electric-field modelling approach for individualized targeting of transcranial magnetic stimulation treatment
- PMID: 34321597
- PMCID: PMC8674270
- DOI: 10.1038/s41386-021-01110-6
Proof of concept study to develop a novel connectivity-based electric-field modelling approach for individualized targeting of transcranial magnetic stimulation treatment
Abstract
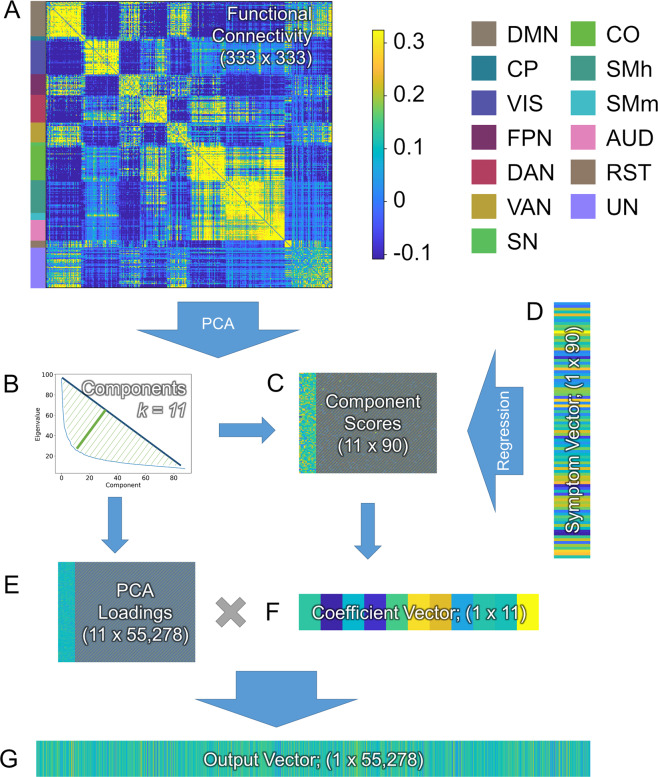
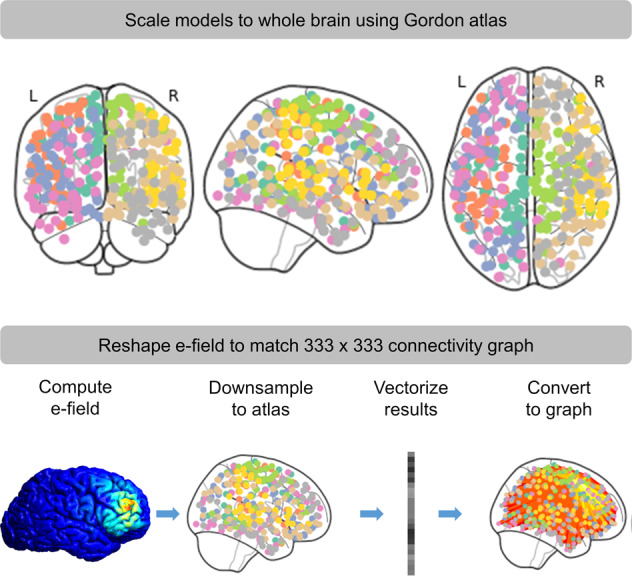
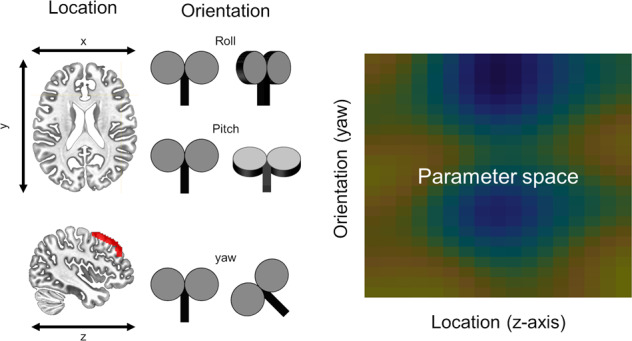
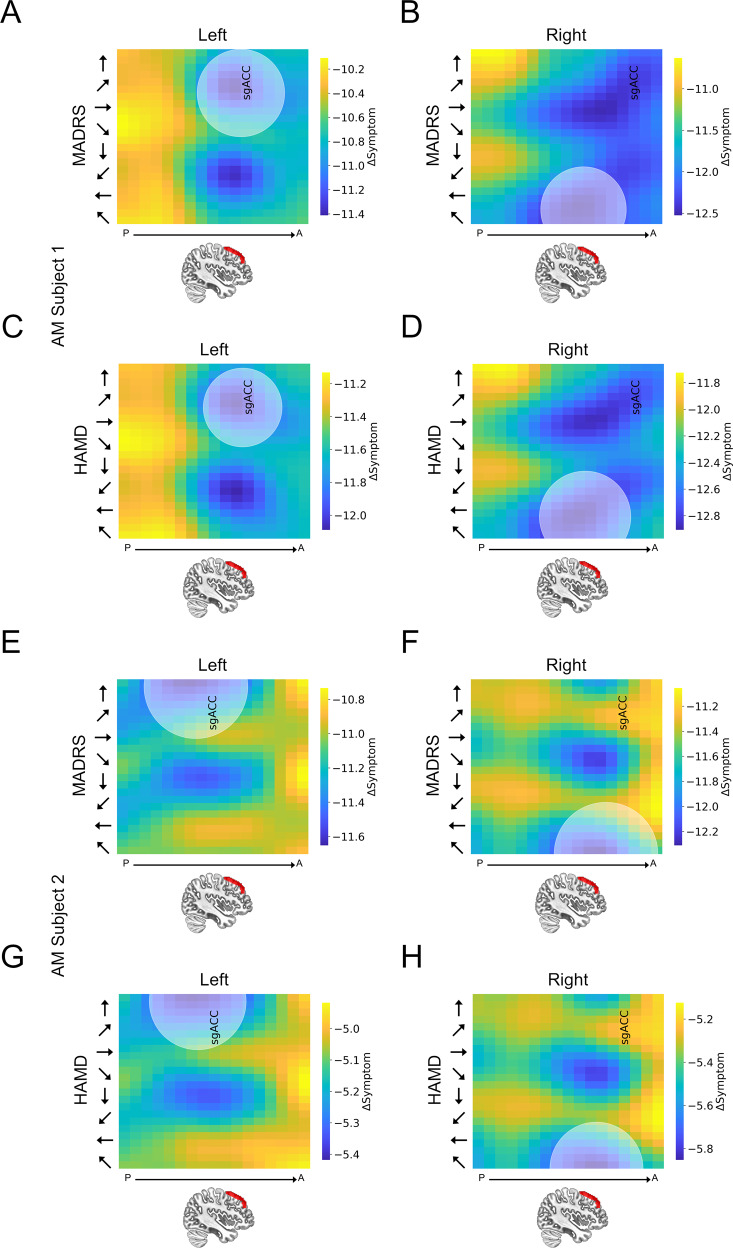
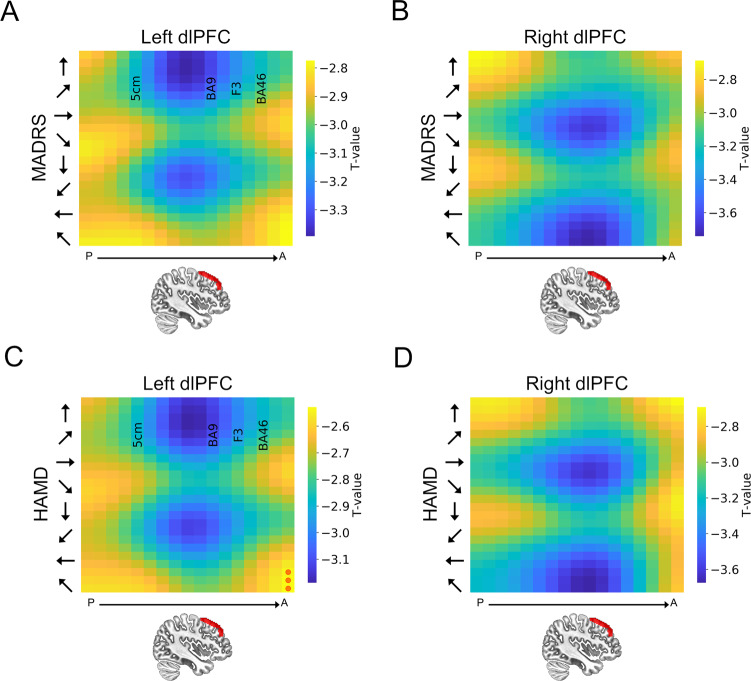
Resting state functional connectivity (rsFC) offers promise for individualizing stimulation targets for transcranial magnetic stimulation (TMS) treatments. However, current targeting approaches do not account for non-focal TMS effects or large-scale connectivity patterns. To overcome these limitations, we propose a novel targeting optimization approach that combines whole-brain rsFC and electric-field (e-field) modelling to identify single-subject, symptom-specific TMS targets. In this proof of concept study, we recruited 91 anxious misery (AM) patients and 25 controls. We measured depression symptoms (MADRS/HAMD) and recorded rsFC. We used a PCA regression to predict symptoms from rsFC and estimate the parameter vector, for input into our e-field augmented model. We modeled 17 left dlPFC and 7 M1 sites using 24 equally spaced coil orientations. We computed single-subject predicted ΔMADRS/HAMD scores for each site/orientation using the e-field augmented model, which comprises a linear combination of the following elementwise products (1) the estimated connectivity/symptom coefficients, (2) a vectorized e-field model for site/orientation, (3) rsFC matrix, scaled by a proportionality constant. In AM patients, our connectivity-based model predicted a significant decrease depression for sites near BA9, but not M1 for coil orientations perpendicular to the cortical gyrus. In control subjects, no site/orientation combination showed a significant predicted change. These results corroborate previous work suggesting the efficacy of left dlPFC stimulation for depression treatment, and predict better outcomes with individualized targeting. They also suggest that our novel connectivity-based e-field modelling approach may effectively identify potential TMS treatment responders and individualize TMS targeting to maximize the therapeutic impact.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- American Psychiatric Association. Anxiety disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). Arlington VA (2013). 10.1176/appi.books.9780890425596.dsm05.
-
- Scott KM, de Jonge, P, Stein DJ & Kessler RC Mental disorders around the world: Facts and figures from the WHO World Mental Health surveys. Mental Disorders Around the World: Facts and Figures from the WHO World Mental Health Surveys (2018). 10.1017/9781316336168
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
